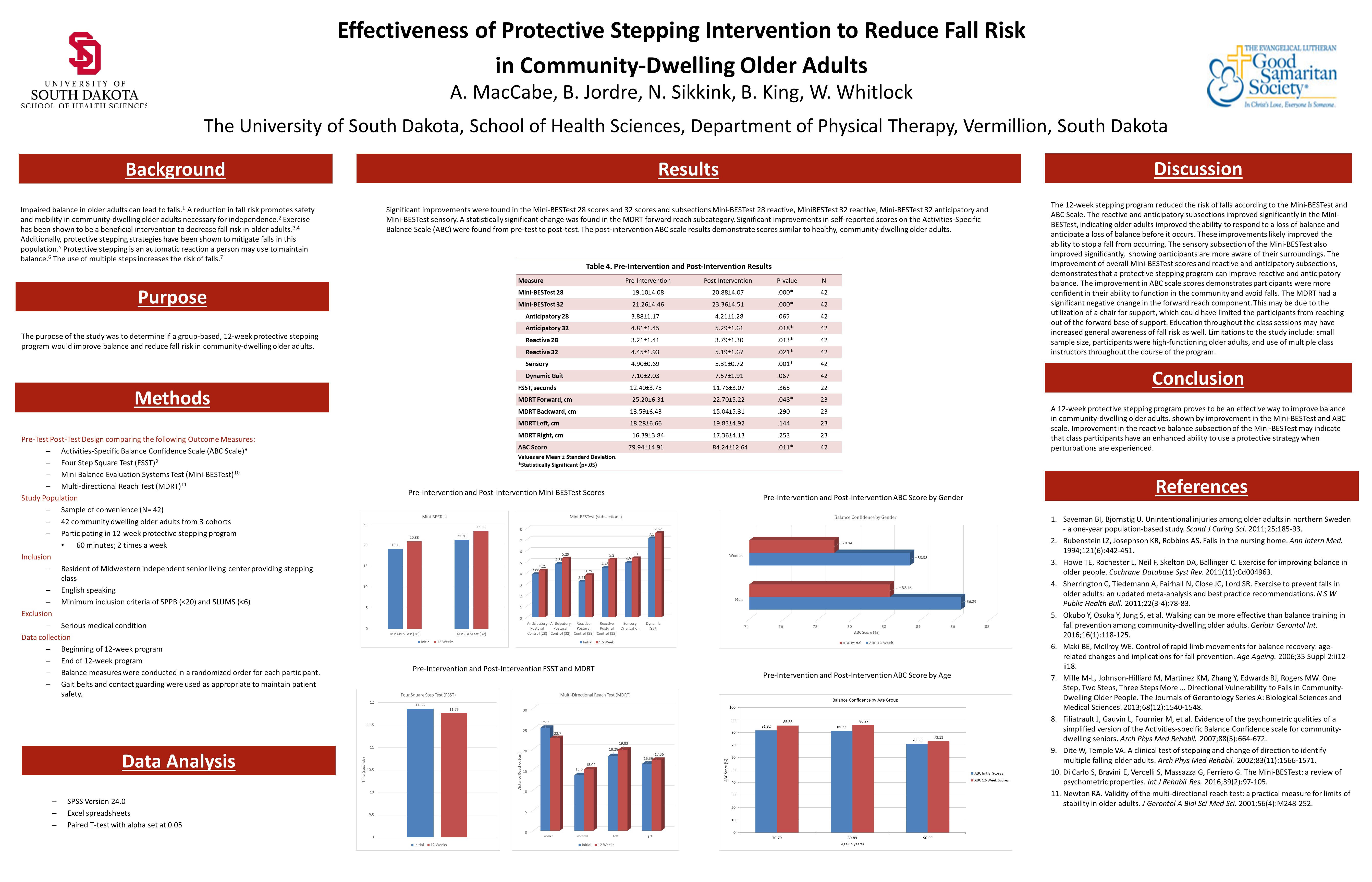
Effectiveness of Protective Stepping Intervention to Reduce Fall Risk in Community-Dwelling Older Adults
Nicole Sikkink, SPT, Beth King, SPT, and Will Whitlock, SPT
(Click on image to expand)
Nicole Sikkink, SPT, Beth King, SPT, and Will Whitlock, SPT
(Click on image to expand)

1. Was there any correlation(s) that you found between the increase in overall balance and the actual number of falls in this cohort?
2. Was there any gender differences with increased balance, or overall decrease of fall risk?
LikeLike
In our study, we primarily focused on analyzing the pre-intervention data of each outcome measure vs. the post-intervention data of each outcome measure. We did not necessarily look at overall balance, but more specifically the improvements in the outcome measures which each look at different parts of balance such as reactive balance, anticipatory balance, and confidence with balance when performing certain activities. Looking at correlations between the increase in overall balance and actual number of falls would be a great addition to this study or future research.
We did not look at specific gender difference due to the majority of our participants being female and the overall small sample size. We did look at Pre and Post intervention balance confidence by specific gender, but we did not compare them.
Thank you for the questions, Niccole!
LikeLike
Thanks for doing this research! It appears based on your results that a stepping program would be a great thing to incorporate in the community and living spaces to help prevent fall risks in older adults. What are some the barriers that you see may potentially make the implementation of these stepping programs difficult? Another question I have is regarding the exclusion criteria. It states that participants were excluded based on a serious medical condition so I was just wondering how you determined the seriousness of a medical condition?
I enjoyed seeing what you found in your study!
LikeLike
Thanks for your questions, Justine! Some of the barriers that may make the implementation of this type of program difficult is the availability of space for the classes to be held and coordinating an instructor or instructors, whether it is a physical therapist or any other qualified individual. In regards to the serious medical condition, participants were excluded if they had a serious medical condition deemed dangerous for participation by the independent living facility. So that exclusion criterion was up to the independent living facility and their responsibility to keep participants safe during the classes rather than up to us, the researchers.
LikeLike
Justine: Thank you for your questions. As it pertains to barriers to incorporating a stepping program, we strongly believe that designing a stepping program for community-dwelling older adults in this facility would be most cost-effective w/ an activities coordinator. The ideal outcome from a group stepping program would be to reduce the risk of falls for the most people. Thus, as Beth stated, having the necessary resources to do so is very important. Ideally, a licensed physical therapist would be there to lead the class, but financially that just is not plausible some of the time, especially in this case. With that said, there are many PT group therapy facilities around the nation specializing in falls, Parkinson’s disease, and other patient-specific diagnoses. I believe it would be interesting to compare the outcomes from a “layperson” leading a stepping class as opposed to a licensed physical therapist!
LikeLike
I noticed you had exclusion criteria of serious medical conditions. What do you think the results would be like if you had included participants or looked a certain disease? Also what made you select the balance measures you did? Thanks for the information!
LikeLike
Holly,
Thank you for your question! First off, we excluded participants with serious medical conditions from our research study because we were looking for our participants to exemplify the “community-dwelling older adults” category. We felt that those with serious medical conditions would not be appropriate for our intended sample. Also, I truly believe that this research study could be done on a specific population; such as those with Parkinson’s disease. Most geriatrics participating in a stepping/balance program could benefit immensely from balance training, thus reducing fall risk!
Secondly, we carefully selected our balance measures through rigorous research and statistical analyses to find those most appropriate for our intended population (community-dwelling older adults) and our intended variable (balance). The balance measures we have chosen have proven to be valid, reliable, well-researched, and formal enough to execute on a consistent basis w/o a lot of opportunity for interrater/intrarater issues. I’m sure there are many other balance measures that would work great for this population! It must be noted that time/resources played a factor as well.
LikeLike
Hi, I have to say you all made a great poster and presented it very well. I have two questions, first you did find significant improvements suggesting a decrease in fall risk. Through your research are the changes you found clinically significant? Second, did you find any literature on the dosing required for most balance/exercise programs to show a clinically significant improvement. Lastly, was the frequency and duration of the program based upon evidence in the literature for dosing or was it more so ease of schedule/implementation etc.
Thanks for your time.
LikeLike
Hi Kyle! Thanks for your questions about our research. I will answer your first question and let the other two PT students in my research group answer the other! You are correct; we found statistically significant improvements that suggest a decrease in fall risk after participation in a protective stepping program. The independent living facility that conducted the class utilized what we found in our research to determine if they would continue with the class and expand to other facilities. Since we found statistically significant improvements suggesting a decrease in fall risk, the independent living facility has decided to move forward with the class. I would say that this shows that the results were clinically significant.
LikeLike
Thanks Kyle. As Beth mentioned, the independent living facility that conducted the classes wanted us to conduct the research to see the effectiveness of this program and therefore continue the class in other facilities. Our literature review primarily focused on what outcome measures would be the best for this population to show a change and then help this facility determine whether or not this change was big enough to continue in other facilities. The program consisted of 2 classes, 12 times a week. It included different stepping movements, sit to stand, and other exercises to improve balance reactions. The class was taught by an employee within the facility, they did not have to meet specific criteria to teach the class. The program was already made when we started this study, with that, I would say that the frequency and duration of the class was a little of both – ease of schedule/ implementation as well as based on evidence. We did find significant improvements in balance from the class which tells us that the dosing and frequency of this program specifically was effective. I hope this clears up your question a little.
LikeLike
*** Sorry, I meant to say the program was 2 times a week for 12 weeks (not 2 classes 12 times a week)**
LikeLike
I like how you used the center of your poster to display all of your results as tables, it is easy to read and looks very nice! Did you look for any participant variables associated with greater changes in results? Since there is such a wide range of abilities in community dwelling older adults, I am wondering if there is a subset that your intervention program would be most useful for. For instance, maybe community members who had lower or mid-range pretest scores benefited more than those with high scores due to a possible ceiling affect. It would also make sense if those with very low pretest scores benefited little due to an inability to fully participate in a group program. Did you notice any trends such as these in your data? I could see this type of information being useful for prescription of exercise programs specific to our patients.
LikeLike
Thanks for the question, Jessie!
In this research project, we looked at the participant population as a whole, not subgroups of the different variables. We primarily chose to focus on this because of the small sample sizes therefore, lacking the strength to generalize the data. I agree, there is such a wide variety of function and abilities in community dwelling adults. With that being said, the SPPB and SLUM tests were conducted to make sure the participants were safe and capable of following along with the class.
The SPPB test determines the level of LE strength, gait speed, and balance of a community dwelling adults, but is not the best at capturing function in higher functioning patients. Since we compared pre test vs. post test, the change between each individual’s score was calculated and then we determined whether it was a significant change or not. In doing this, we were hoping to minimize the ceiling effect of the higher scoring pretest scores. The main goal of our study was to see if a general stepping class would benefit this population as a whole, not specific levels of functioning within this group.
I hope that this answered your question! Thanks!
LikeLike
Hi, great job on the study and poster! I just have a question regarding the protective stepping program that was utilized. What were some of the exercises and progressions throughout the program applied? Was it a combination of proprioceptive exercises and strengthening exercises? Since it was a class, were exercises performed as a group or were exercises specific to each participant’s level of function?
LikeLike
Thanks for your questions Steven! The program mainly consisted of stepping patterns (such as diagonal, to the side, and backward) while standing behind a chair for support. These stepping patterns were used to help participants feel more comfortable using a step in different directions should they need to use a stepping strategy to prevent a fall. The program also utilized sit-to-stand sequences along with some other general movements and stretches for community dwelling older adults. Unfortunately, we were not able to observe a full class session, but we received the PDF documents that explained the class set up and progressions. The exercises were performed as a group and were not specific to each participant’s level of function, although participants could make some modifications based on their ability and safety was always most important.
LikeLike
Very beneficial study! I also appreciated the display of the data. Just a few things that crossed my mind as I was reading your research: 1) Were any of these participants utilizing assistive devices or were those individuals excluded from the study? Just curious as to what their assistance baseline was prior to the stepping program. 2) You also mentioned that there was a decrease in the MDRT and FSST scores due to increased awareness through education they received during the stepping program. What did the educational sessions consist of?
Last question! Are there plans to do any follow-up testing with these individuals to track their performance and falls to better determine long-term program retention?
Great work, guys! It was an interesting read. Thanks!
LikeLike
Avery, excellent question on the assistive devices utilized during our research. As a matter of fact, we included all subjects that were deemed “community-dwelling” in our research, regardless of assistive device use or not. I must say, it was rather difficult for subjects utilizing a FWW during the FSST testing due to the obvious setback they were put at prior to participating. For those that were able, we most often just had the subject place their assistive device to the side if they were comfortable completing the FSST without it. Most of our patients participating in the research did not use an assistive device. Also, if patients participating in the research were deemed to be unsafe for the group stepping class, they were excluded from the research. A sort of pre examination that our subjects were required to pass prior to being included in the research.
LikeLike
Great poster and information! In the poster, you stated that education that was provided throughout the class sessions may have increased the participants overall awareness of fall risks. Could you explain a little bit more about what kind of education was provided? Also, was there education provided at every session? Thanks!
LikeLike
Looks like Avery and I posted similar questions at the same time! Let me add to mine. Did you give the instructor any sort of script or protocol for providing education? And if so, how did you choose what to educate the participants about?
LikeLike
Thanks for your questions Maggie! We did not provide the instructor with a script for providing education, as this class was created by professionals within the independent living facility and they just wanted us to research the effectiveness of the program they had initiated. The instructors did have a handout that guided them through the class with verbal cues to use. I believe education as provided as needed as participants asked questions or as exercises were performed. The point of any education provided was to increase awareness of falls and how to prevent them.
LikeLike
Hey all! Sorry for the late question. Great study and poster as it pertains to improving the health, safety, and independence of our geriatric populations within the community. There has been a lot of great questions addressed. Looking back at my research project, there are a few things I would change. What is the one thing that you guys would change or improve upon in your study?
Thanks!
LikeLike
Hey Colton! Thanks for the question. The obvious answer right off the bat is that we would have gathered a larger sample size for the research. Our research data spans over 3 years of PT classes and faculty research advisors, so more years to gather more data from “community-dwelling older adults” would have been ideal. As for a factor that we could control ourselves, we would have liked to have gathered a more thorough patient history prior to our patients participating in our research. This would have allowed us toAlso, we would have really enjoyed, at the bare minimum, being a part of the group stepping class to see how the class is organized. It would have also been interesting to see how our subjects performed in the group stepping class to gauge active participation!
LikeLike
Avery, excellent question on the assistive devices utilized during our research. As a matter of fact, we included all subjects that were deemed “community-dwelling” in our research, regardless of assistive device use or not. I must say, it was rather difficult for subjects utilizing a FWW during the FSST testing due to the obvious setback they were put at prior to participating. For those that were able, we most often just had the subject place their assistive device to the side if they were comfortable completing the FSST without it. Most of our patients participating in the research did not use an assistive device. Also, if patients participating in the research were deemed to be unsafe for the group stepping class, they were excluded from the research. A sort of pre examination that our subjects were required to pass prior to being included in the research.
LikeLike
Hello, I would first like to say that this is a great poster presentation! It is informative, clear, and well formatted. I just have one question. The study population is stated as “community dwelling older adults,” was there a certain age range you looked at for inclusion? For example >65 years old. My thought is that having a specific age range may increase applicability and significance in relationship to other studies. Thank you!
LikeLike