Jennifer Hall, SPT, Shelbi Hatfield, SPT, Sarah Moen, SPT, and Alyssa Pfeifle, SPT
27 Comments on “IFSP Rating Scale”
What do you feel is the biggest drawback/downfall of the IFSP and what would you propose to specifically address that issue if the IFSP were to be revised? Thank you.
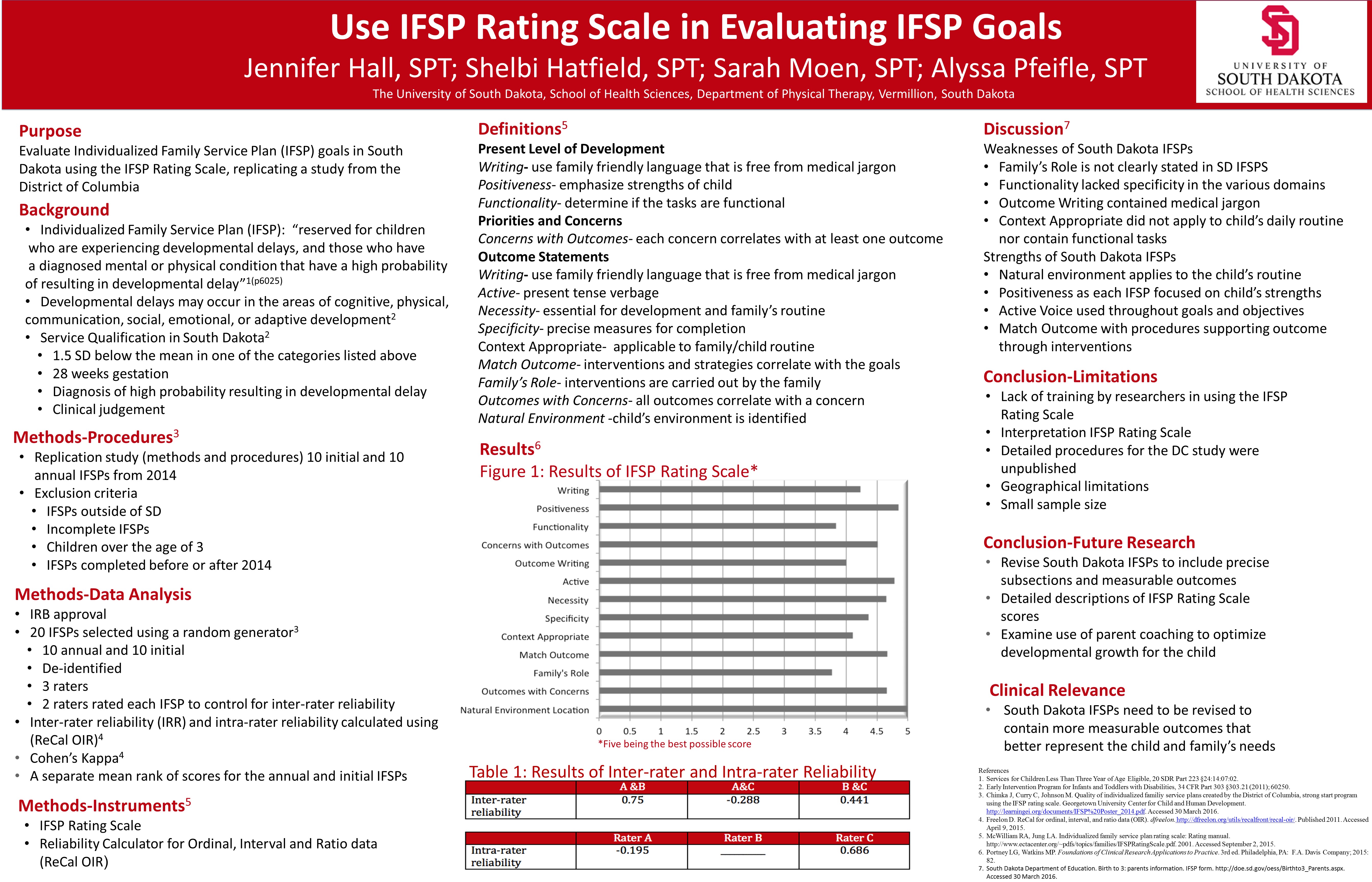
I don’t believe the IFSP itself has a specific drawback, I would say the drawback comes when each state fills out their IFSP differently. For example, the District of Columbia filled out the IFSP using measurable outcomes and usually specifying parent involvement while the South Dakota IFSPs were generally not very measurable and parental involvement was implied instead of specified. My recommendation would be that all states fill out the IFSP the same using the above outcome statements in Figure 1.
I agree with Shelbi and Sarah on the greatest drawback to IFSPs in South Dakota especially changing the IFSP form itself and writing measurable goals. I’ve been working in The Birth to Three program in my current rotation, and I have found that Nebraska and other states are implementing RBI which stands for routine based interview. The RBI asks open-ended questions and goes through the step by step process of each activity during the day from waking up to going to bed. Additionally, it allow the parents to voice their thoughts instead of the provider putting thoughts in their head by guiding them with close-ended questions. Currently this is not required in every state, however, I believe that making this process mandatory is essential in order for providers to understand the needs, goals, and challenges of the family. Then after completing the RBI, the provider has a thorough understanding of the family and can picture their daily routine which enables them to write family-centered, measurable goals and address their needs.
I would propose the SD IFSP forms have more measurable goals to allow the therapists, the birth to three coordinators, and the parents to specifically see when the developmental goals were achieved. This would also create easier IFSP review meetings by allowing the therapist to gauge the child’s progress towards meeting the goal. The challenge with the SD form is that there is no measurable checklist, chart, or optional goals that a therapist can base a goal off of.
Barriers between therapist and parent are also creating difficult family role outcomes. Barriers could include socio-economic status (parents may not have sensory stimulating toys), language differences, learning difficulties, cognitive status differences, time management difficulties, etc. SD is looking to implement a more “parent centered therapy” allowing parents to complete most of the therapy for the child and decreasing the role therapists will have. However, I feel that example barriers listed above will slow or keep SD from fully implementing this option. Therefore, family role is still considered as a downfall to SD IFSPs. (I learned more information on SD’s Birth to Three plans at my clinical in Aberdeen. It’s hard to explain it all in a short comment and again it is only in the experimental stages. Again this is mostly what I saw in the clinic and what I have heard)
I agree with what Sarah, Jen, and Shelbi stated. I feel like one of SD IFSP’s largest drawbacks is that the goals do not need to be measurable making it difficult to determine whether the goal has actually been met or not. If a goal is not required to be measurable, it is up for therapist interpretation to determine whether the child has met the goal or not which can lead to difficulties if a child has a fill-in therapist as one PT may feel like the child met the goal and the other PT may feel like the goal was not met.
Another drawback I feel like is that SD IFSPs have an optional section that is not required to be completed. If the IFSP was to be revised, I think the optional section should become mandatory as it gives the therapist a better idea about what the family’s needs are.
One of the limitations is lack of training in using the IFSP. What are some of the best ways to efficiently and effectively train therapists to use the IFSP? Is a form of standardized training necessary?
I believe an online training module would be the easiest and most efficient way to use the IFSP. This would allow therapist in all locations, whether rural or urban, to complete the training with the ease of a computer. It could be a quick 2 hour information module that explains the different areas of the IFSP form and give examples per section of what is desired to be written. This would allow all therapists in SD to receive the same formal training prior to documenting for the state. Consequently, there can only be one standardized training per state because each state’s IFSP form is slightly different.
Like Sarah said I think some type of IFSP training is necessary whether it be online or in person before a PT is allowed to work as a birth to three provider. By having providers go through a standardized training, each provider will know exactly how to use the form and what the state’s expectations are for completing the form. To create the training module, SD should create a task force of experienced birth to three providers who have experience utilizing the IFSP form. These providers will understand what challenges face new birth to 3 providers for using the IFSP form and what areas they frequently see lacking information.
As I previously mentioned above, the routine based interview (RBI) would be an excellent tool for providers to get information from the family for the IFSP. Then in order for the providers to place this information in the IFSP, a training module as Sarah explain would be very useful. I think that this should be standardized training that all providers are required to obtain before becoming birth to three providers, but first it would have to pass at the state level and then the national level.
It would be wonderful if the IFSP was standardized across the U.S., however since its not; providers should attend all meetings associated with the IFSP format and changes for the current state they are practicing in. For our research we contacted the USD Center for Disabilities to get more information about IFSPs and obtain our de-identified IFSPs. Each state should have an organization that is charge of IFSPs or a website that providers can obtain more information about IFSPs for their specific state.
As alyssa mentioned above, IFSPs are not standardized across the US so training in the use of an IFSP would have to be by each state. However, standardizing the IFSP would make for much easier training in its use. I also agree with what sarah mentioned of an online module or having to take continuing education courses on the IFSP should be required to be a birth to three provider in every state. If all birth to three providers were educated in the IFSP rating scale and how the IFSP should be written, outcomes would be more effective for providers and the children.
One of the biggest differences was that DC included an entire section to parental involvement to help the child reach their individual goals. Another big difference was that DC made all their goals specific and measurable while SD did not do this. Those were the biggest things we saw when replicating the DC study.
We did not explore the reasons for the differences in our research. We did however compare the forms. We noticed that the DC form had mandatory pages where the SD form had multiple pages that were optional. It’s unclear if these optional pages would make the gap between states more comparable or not. However, it is a possibility to consider. Individual state training may also contribute to these differences. More research needs to be done to find a clear explanation.
As Sarah and Shelbi mentioned, the biggest weakness comes from the lack of detail especially when talking about measurable goals.Here is a specific example. In DC IFSP form there are sections that enable the therapist to create goals that easily integrate into the family’s routine and priorities by specifically asking the family to complete sections on family leisure activities. In contrast, SD IFSP form only includes optional content sections for family priorities and activities. Additionally, DC IFSP form also uses a quantitative method to evaluate outcome measures and goals by rating the level of completion, whereas the SD IFSP form does not.
Did you happen to discover how the strengths of IFSPs correlate with good school systems, or vice versa? If not, do you think there would be a correlation between a good school district and the strengths of IFSPs in that school district?
Actually IFSPs are not with the school district, you must be thinking of IEPs. IFSPs are for children from birth to three years old. A future research project could look at IEPs and school district’s but I believe the results would be contingent on the state’s information/training and not the schools, just as in the IFSPs.
Like Sarah said below, IFSPs do not correlate with school districts as these are for children under the age of 3. I do think it would be interesting to look at though how the strength of the IFSP correlated to different regions of the state as we only looked at IFSPs from the Sioux Falls area. It would be interesting to see how IFSPs completed in Sioux Falls compared to IFSPs completed in Rapid City to IFSPs completed in smaller cities in the state.
I think parental involvement should be addressed. I know South Dakota birth to three services is trying to work through this issue right now. I just feel that going into the homes most parents would be on their phones and not watching to learn how to help their child progress. Therapists also go into day cares where parents aren’t even there. This makes it difficult for daily carry over and for a child to progress. Research needs to be done to achieve a balance of therapist direct/assistance and patent autonomy.
I think research in this field should go to showing birth to three providers the IFSP rating scale and educating them on how to use the scale to fill out and make better goals on the IFSPs they complete. This would lead to better outcomes for the children.
The inter-rater and intra-rater reliability among the three researchers seems to be all over the place. Do you think this is an accurate representation of reliability among all clinicians, or can it be attributed to being novice raters?
It was definately due to being novice raters. We did not have an formal training prior to rating. So my rating opinions were different than the other two raters. It was a challenge we definately faced.
I think the inter-rater reliability can partially be related to being novice raters as we, like Sarah said, had no previous training prior to utilizing the rating scale. I also think part of the large differences found in inter-rater reliability can be contributed to rater interpretation on some of the categories of the scale. One of the categories on the rating scale was medical jargon depending on whether the rater believed medical jargon was used in the IFSP or not affected the ratings significantly. An example of this that we found in our study was midline. Two raters felt like midline was medical jargon and scored that section a 1 while one rater did not feel like midline was medical jargon and scored the section a 5 leading to wide variations in our scoring.
I believe part of the wide variances that we saw in intra-rater reliability was due to the time between ratings. We initially did not look at intra-rater reliability so there were a couple weeks between our initial rating and the second rating. If we were to redo this study, I think looking at intra-rater reliability initially would be important.
I also believe that the inter and intra rater reliability is due not being trained with the IFSP Rating Scale. As Alyssa mentioned, each grader interpreted sections and meanings differently. More education on how to use the scale and a better understanding of grading the IFSP using the scale are needed.
I wish I had more experience with this to give wise input but reading all of these above is very enlightening and obvious you have raised some real concerns that can be addressed. Biggest thing I would like to see in your poster presentation is an ending paragraph on “Where do we go from here?” – especially now that you have received such insightful feedback from so many.
Thanks for your response Scott. As you mentioned we hope that this research provides some insight on ways to change the current IFSP form in South Dakota, but we need to generate support and awareness about this issue in order for the policy makers to make changes to it.
Great question Scott! Because IFSP’s are state designed legal documents, in accordance with the Federal Law, the next step was to share the results with the policy makers in SD. And this has been done to the Birth to Three overseers.

What do you feel is the biggest drawback/downfall of the IFSP and what would you propose to specifically address that issue if the IFSP were to be revised? Thank you.
LikeLiked by 1 person
I don’t believe the IFSP itself has a specific drawback, I would say the drawback comes when each state fills out their IFSP differently. For example, the District of Columbia filled out the IFSP using measurable outcomes and usually specifying parent involvement while the South Dakota IFSPs were generally not very measurable and parental involvement was implied instead of specified. My recommendation would be that all states fill out the IFSP the same using the above outcome statements in Figure 1.
LikeLiked by 1 person
I agree with Shelbi and Sarah on the greatest drawback to IFSPs in South Dakota especially changing the IFSP form itself and writing measurable goals. I’ve been working in The Birth to Three program in my current rotation, and I have found that Nebraska and other states are implementing RBI which stands for routine based interview. The RBI asks open-ended questions and goes through the step by step process of each activity during the day from waking up to going to bed. Additionally, it allow the parents to voice their thoughts instead of the provider putting thoughts in their head by guiding them with close-ended questions. Currently this is not required in every state, however, I believe that making this process mandatory is essential in order for providers to understand the needs, goals, and challenges of the family. Then after completing the RBI, the provider has a thorough understanding of the family and can picture their daily routine which enables them to write family-centered, measurable goals and address their needs.
LikeLiked by 1 person
I would propose the SD IFSP forms have more measurable goals to allow the therapists, the birth to three coordinators, and the parents to specifically see when the developmental goals were achieved. This would also create easier IFSP review meetings by allowing the therapist to gauge the child’s progress towards meeting the goal. The challenge with the SD form is that there is no measurable checklist, chart, or optional goals that a therapist can base a goal off of.
Barriers between therapist and parent are also creating difficult family role outcomes. Barriers could include socio-economic status (parents may not have sensory stimulating toys), language differences, learning difficulties, cognitive status differences, time management difficulties, etc. SD is looking to implement a more “parent centered therapy” allowing parents to complete most of the therapy for the child and decreasing the role therapists will have. However, I feel that example barriers listed above will slow or keep SD from fully implementing this option. Therefore, family role is still considered as a downfall to SD IFSPs. (I learned more information on SD’s Birth to Three plans at my clinical in Aberdeen. It’s hard to explain it all in a short comment and again it is only in the experimental stages. Again this is mostly what I saw in the clinic and what I have heard)
LikeLiked by 1 person
I agree with what Sarah, Jen, and Shelbi stated. I feel like one of SD IFSP’s largest drawbacks is that the goals do not need to be measurable making it difficult to determine whether the goal has actually been met or not. If a goal is not required to be measurable, it is up for therapist interpretation to determine whether the child has met the goal or not which can lead to difficulties if a child has a fill-in therapist as one PT may feel like the child met the goal and the other PT may feel like the goal was not met.
Another drawback I feel like is that SD IFSPs have an optional section that is not required to be completed. If the IFSP was to be revised, I think the optional section should become mandatory as it gives the therapist a better idea about what the family’s needs are.
LikeLiked by 1 person
One of the limitations is lack of training in using the IFSP. What are some of the best ways to efficiently and effectively train therapists to use the IFSP? Is a form of standardized training necessary?
LikeLiked by 1 person
I believe an online training module would be the easiest and most efficient way to use the IFSP. This would allow therapist in all locations, whether rural or urban, to complete the training with the ease of a computer. It could be a quick 2 hour information module that explains the different areas of the IFSP form and give examples per section of what is desired to be written. This would allow all therapists in SD to receive the same formal training prior to documenting for the state. Consequently, there can only be one standardized training per state because each state’s IFSP form is slightly different.
LikeLiked by 1 person
Like Sarah said I think some type of IFSP training is necessary whether it be online or in person before a PT is allowed to work as a birth to three provider. By having providers go through a standardized training, each provider will know exactly how to use the form and what the state’s expectations are for completing the form. To create the training module, SD should create a task force of experienced birth to three providers who have experience utilizing the IFSP form. These providers will understand what challenges face new birth to 3 providers for using the IFSP form and what areas they frequently see lacking information.
LikeLiked by 1 person
As I previously mentioned above, the routine based interview (RBI) would be an excellent tool for providers to get information from the family for the IFSP. Then in order for the providers to place this information in the IFSP, a training module as Sarah explain would be very useful. I think that this should be standardized training that all providers are required to obtain before becoming birth to three providers, but first it would have to pass at the state level and then the national level.
It would be wonderful if the IFSP was standardized across the U.S., however since its not; providers should attend all meetings associated with the IFSP format and changes for the current state they are practicing in. For our research we contacted the USD Center for Disabilities to get more information about IFSPs and obtain our de-identified IFSPs. Each state should have an organization that is charge of IFSPs or a website that providers can obtain more information about IFSPs for their specific state.
LikeLiked by 1 person
As alyssa mentioned above, IFSPs are not standardized across the US so training in the use of an IFSP would have to be by each state. However, standardizing the IFSP would make for much easier training in its use. I also agree with what sarah mentioned of an online module or having to take continuing education courses on the IFSP should be required to be a birth to three provider in every state. If all birth to three providers were educated in the IFSP rating scale and how the IFSP should be written, outcomes would be more effective for providers and the children.
LikeLiked by 1 person
What contributed to the differences between the D.C. IFSPS and the SD ones?
LikeLiked by 1 person
One of the biggest differences was that DC included an entire section to parental involvement to help the child reach their individual goals. Another big difference was that DC made all their goals specific and measurable while SD did not do this. Those were the biggest things we saw when replicating the DC study.
LikeLiked by 1 person
We did not explore the reasons for the differences in our research. We did however compare the forms. We noticed that the DC form had mandatory pages where the SD form had multiple pages that were optional. It’s unclear if these optional pages would make the gap between states more comparable or not. However, it is a possibility to consider. Individual state training may also contribute to these differences. More research needs to be done to find a clear explanation.
LikeLiked by 1 person
As Sarah and Shelbi mentioned, the biggest weakness comes from the lack of detail especially when talking about measurable goals.Here is a specific example. In DC IFSP form there are sections that enable the therapist to create goals that easily integrate into the family’s routine and priorities by specifically asking the family to complete sections on family leisure activities. In contrast, SD IFSP form only includes optional content sections for family priorities and activities. Additionally, DC IFSP form also uses a quantitative method to evaluate outcome measures and goals by rating the level of completion, whereas the SD IFSP form does not.
LikeLiked by 1 person
Did you happen to discover how the strengths of IFSPs correlate with good school systems, or vice versa? If not, do you think there would be a correlation between a good school district and the strengths of IFSPs in that school district?
LikeLiked by 1 person
Actually IFSPs are not with the school district, you must be thinking of IEPs. IFSPs are for children from birth to three years old. A future research project could look at IEPs and school district’s but I believe the results would be contingent on the state’s information/training and not the schools, just as in the IFSPs.
LikeLiked by 1 person
Like Sarah said below, IFSPs do not correlate with school districts as these are for children under the age of 3. I do think it would be interesting to look at though how the strength of the IFSP correlated to different regions of the state as we only looked at IFSPs from the Sioux Falls area. It would be interesting to see how IFSPs completed in Sioux Falls compared to IFSPs completed in Rapid City to IFSPs completed in smaller cities in the state.
LikeLiked by 1 person
Where do you believe research in this field needs to be directed to next?
LikeLiked by 1 person
I think parental involvement should be addressed. I know South Dakota birth to three services is trying to work through this issue right now. I just feel that going into the homes most parents would be on their phones and not watching to learn how to help their child progress. Therapists also go into day cares where parents aren’t even there. This makes it difficult for daily carry over and for a child to progress. Research needs to be done to achieve a balance of therapist direct/assistance and patent autonomy.
LikeLiked by 1 person
I think research in this field should go to showing birth to three providers the IFSP rating scale and educating them on how to use the scale to fill out and make better goals on the IFSPs they complete. This would lead to better outcomes for the children.
LikeLiked by 1 person
The inter-rater and intra-rater reliability among the three researchers seems to be all over the place. Do you think this is an accurate representation of reliability among all clinicians, or can it be attributed to being novice raters?
LikeLiked by 1 person
It was definately due to being novice raters. We did not have an formal training prior to rating. So my rating opinions were different than the other two raters. It was a challenge we definately faced.
LikeLiked by 1 person
I think the inter-rater reliability can partially be related to being novice raters as we, like Sarah said, had no previous training prior to utilizing the rating scale. I also think part of the large differences found in inter-rater reliability can be contributed to rater interpretation on some of the categories of the scale. One of the categories on the rating scale was medical jargon depending on whether the rater believed medical jargon was used in the IFSP or not affected the ratings significantly. An example of this that we found in our study was midline. Two raters felt like midline was medical jargon and scored that section a 1 while one rater did not feel like midline was medical jargon and scored the section a 5 leading to wide variations in our scoring.
I believe part of the wide variances that we saw in intra-rater reliability was due to the time between ratings. We initially did not look at intra-rater reliability so there were a couple weeks between our initial rating and the second rating. If we were to redo this study, I think looking at intra-rater reliability initially would be important.
LikeLiked by 1 person
I also believe that the inter and intra rater reliability is due not being trained with the IFSP Rating Scale. As Alyssa mentioned, each grader interpreted sections and meanings differently. More education on how to use the scale and a better understanding of grading the IFSP using the scale are needed.
LikeLiked by 1 person
I wish I had more experience with this to give wise input but reading all of these above is very enlightening and obvious you have raised some real concerns that can be addressed. Biggest thing I would like to see in your poster presentation is an ending paragraph on “Where do we go from here?” – especially now that you have received such insightful feedback from so many.
LikeLiked by 1 person
Thanks for your response Scott. As you mentioned we hope that this research provides some insight on ways to change the current IFSP form in South Dakota, but we need to generate support and awareness about this issue in order for the policy makers to make changes to it.
LikeLike
Great question Scott! Because IFSP’s are state designed legal documents, in accordance with the Federal Law, the next step was to share the results with the policy makers in SD. And this has been done to the Birth to Three overseers.
LikeLike