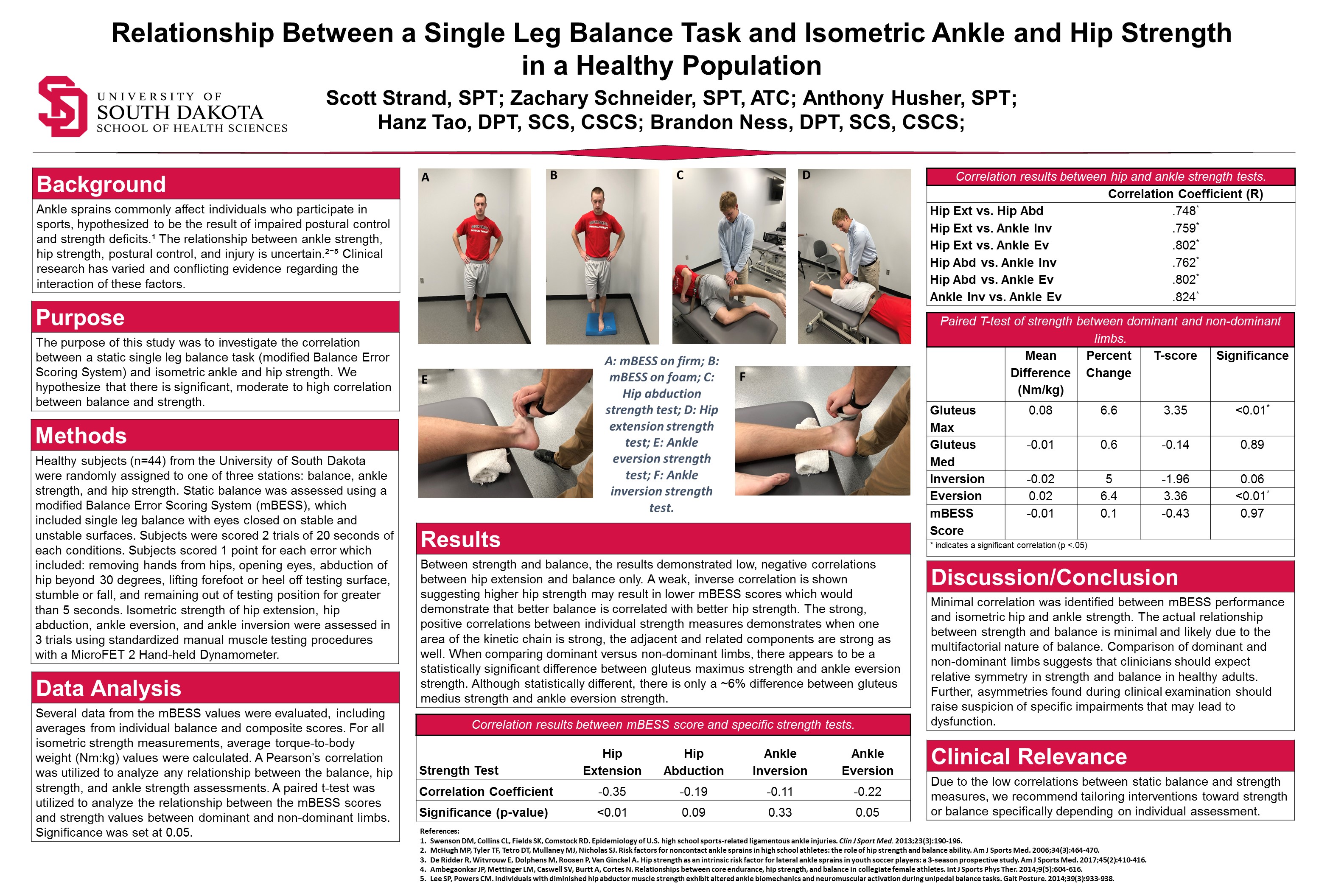
Relationship Between a Single Leg Balance Task and Isometric Ankle and Hip Strength in a Healthy Population
Scott Strand, SPT, Zachary Schneider, SPT, and Anthony Husher, SPT
(Click on image to expand)
Scott Strand, SPT, Zachary Schneider, SPT, and Anthony Husher, SPT
(Click on image to expand)

Do you anticipate that the correlation between strength and dynamic balance assessments would be different than what you found with a static balance assessment? And how would that change the clinical relevance of your results (or not)? Thanks!
LikeLike
Thanks for the question Abby! To answer your first question, I do not believe that there would be a different correlation between strength and a dynamic balance assessment compared to strength and our static balance assessment. The reason that I am leaning more towards saying no, is that so much of balance comes down to so many other factors such as motor control and the ability for the brain to tell the muscle to activate in the first place. If someone was losing their balance, and their muscles in their ankles and hips have not begun to activate, having more strength wouldn’t necessarily help you in regaining balance. I believe that a dynamic balance task takes overall more body control compared to strength. I hope that answers your first question!
To answer your second questions, I think that having data on this correlation would be beneficial and interesting to look at. We are constantly moving and completing dynamic tasks and more times than not we lose our balance while moving and not only standing still. I think looking at it from a static standpoint is beneficial to start with, but I do think we should also explore the relationship with a dynamic balance task to determine if my initial hypothesis is correct or not. I hope that answered your question!
LikeLike
Great poster guys! It looks very professional and well put together. I was just wondering what lead your research group to choose the specific strength tests and balance tests utilized? Was this based on another study that used hip extension, hip abduction, ankle inversion, and ankle eversion strength, or was this based on your own clinical judgement? Thanks again for the great poster, and I hope all three of you are enjoying your clinicals!
LikeLike
Thanks for the question Shantel. We used these strength tests based on several factors. First, using hand-held dynamometry these strength measures showed moderate to excellent intrarater reliability. Secondly, the specific strength tests were used based on other research which has shown these areas to be weak in the chronic ankle instability (CAI) population. The BESS was used also based on its interrater, intrarater, and test-retest reliability. In future research, we would like to compare our healthy population to a CAI population. We needed to utilize these tests with strong reliability to strengthen the quality of future research when we may not be here to perform the tests ourselves!
LikeLike
Nice work, gentlemen! Regarding your inclusion/exclusion criteria, how did you determine if a subject was healthy? Also, did you include subjects who had a history of ankle sprains as they may have poorer ankle strength and balance?
LikeLike
Good question, Hans. Prior to beginning any data collection, we had the participants fill out questionnaires to determine whether they matched the inclusion/exclusion criteria. We excluded those who were pregnancy, a known balance impairment such as vertigo, cold, unresolved head injuries, etc., and a lower extremity injury in the last 6 months. We used the lower extremity injury as the exclusion criteria to tease out those with chronic ankle instability.
LikeLike
Well done. Since there were minimal correlations between strength and stability, is there any other tests other than the mBESS that you could have used to quantify balance?
LikeLike
Thanks for the question Cooper! There are a variety of other balance assessments that we could have used to quantify balance. A couple examples would be the Star Excursion Balance Test and the Y-Balance Test, both of which are more dynamic in nature. I believe the research group that is following up with this research is utilizing the Y-Balance Test so it will be interesting to see what they find in their results.
LikeLike
Good poster, it is very organized! Based off of what you found, do you think that people who are generally weaker will have unaffected balance (assuming that weakness is the only problem the individual has)? Or if there was anything in the literature on this? I only ask since there was low correlation between strength and balance. If that is the case, it makes me wonder if clinical application could mean that a PT could put a lot of focus into strength training (on a weaker patient) while having minimal concern of injury due to balance issues due to the low correlation. Any thoughts? Thanks!
LikeLike
Hello Blake.
Thank you for your question. I want to preface my response by stating that the literature is not unanimous in concluding that balance and strength are independent. However, based on our results and the results of other several other research groups, it would seem as though you are correct. Simply because a person is relatively weak does not mean they will have poor balance. Weakness does not seem to result in poor balance to an extent. I remember Dr. Berg Poppe teaching us one day in Neuro that you do not need to be very strong to have good balance, but you do need some strength. To put it another way, if an individual is extremely weak (i.e. unable to support their body weight against gravity) then of course they will have poor balance. So minor to moderate strength deficits are probably going to have a limited effect on balance, whereas severe deficits will likely have a great effect. All of the subjects in our study are “healthy” and do not approximate the level of weakness described above. I don’t have strength cut offs for you, but generalizations with gray area, for which I apologize.
In response to the second half of your post, there is quite a bit of literature to support the notion that strength training alone can improve both strength and balance. If you focus a patient’s treatment on strengthening alone, they will likely improve their balance as well which is nice. The recommendation is to asses both if you suspect deficits in either area and then incorporate interventions to specifically address whatever deficits are noted, both if necessary.
Thanks Blake! Let me know if you disagree with anything or have any further questions or comments. Have a great day!
LikeLike
Amazing work gentleman. I understand that you didn’t find much of a correlation between strength and static balance. I wonder if your results would have been different if you would have tested balance using a dynamic test? That is, would you hypothesize that dynamic balance may be more reliant on strength compared to static balance? Let’s say all strength tests remained the same, but you utilized, say, a Lower quarter Y balance test, do you think you may have found more of a positive correlation?
LikeLike
Good questions James. Yes we hypothesize that there will be a higher correlation with a dynamic balance task. The class of 2020 will utilize the Y balance task in their research to study just that. So, it is TBD.
Thank you!
Scott
LikeLike
Scott, Will the class of 2020 be assessing dynamic strength as well as dynamic balance? Or will the same isometric strength testing protocol be administered?
James
LikeLike
James, to attempt to answer your question…
The class of 2020 will compare several things, though correlation may or may not be among them. However, we have tested static balance (mBESS), dynamic balance (mYBT), isometric hip and ankle strength. The time commitment to test isokinetic strength was too much to overcome with our limited resources. Further, this research group also learned about the “face validity” of testing isokinetic ankle inversion/eversion. You may also appreciate the challenges of isokinetically testing hip abduction and gluteus maximus. However, it would be interesting to assess one day if technology catches up. Hope that helps.
Dr. Tao
LikeLike
Great research project! In your background section, it states that the research is inconclusive on the relationship between strength and balance in healthy individuals. I am wondering how the literature influenced your decision to target a healthy population. In our Neuromuscular Physical Therapy class we were told that the research shows no significant relationship between strength and balance in healthy individuals. However, the literature shows that there are great improvements in functional balance in older frail individuals that participate in high resistance strength training. While completing this project did you think of any other populations you would like to target with this research?
LikeLike
Thanks for the great question there Hailey. Initially, our thought was to compare our research to a population with Chronic Ankle Instability. Since we performed our research on a healthy population, I would believe our research could be used to compare to another population with slight changes to the inclusion/exclusion criteria and similar methods. The students in your class are performing a similar project on a specific population of athletics! Our group will be excited to see how our research compares to that population.
LikeLike
Stellar poster gang! I was what your definition of a healthy person in the general population was? Was there some level of baseline fitness required or could sedentary individuals have participated as well as someone who is highly active? I was also curious if you noticed any specifically weak muscle groups with comparison to other factors such as gender or activity level? I know you were looking at the populations as a whole but I was just curious if during your testing you noticed any groups with specific deficits or strengths?
LikeLike
Thanks for the question Zack. To answer your first question, our inclusion criteria to be considered our “healthy” individual was that they had to score a 5 or greater on the Tegner Activity Scale, and they could not have any know balance impairments or a lower extremity injury within the previous 6 months. The Tenger Activity Scale is a scale from 0-10, where 0 is no activity up to 10 which is competitive sports at the national level. A Tegner score of 5 indicates that they compete in recreational sports or other physical activity at least twice per week. To answer your second questions, we did not specifically test to determine if there were any weak muscle groups compared to various factors such as gender or age. I myself was in charge of ankle strength, and I did not see any major differences that stood out to be. I am unable to speak for Scott who completed the hip strength testing. Hope that answers your question, thanks!
LikeLike
Great poster!! I was just curious about your criteria for your this study. What personal characteristics and/or conditions did you attempt to exclude? (i.e. previous ankle sprains, vestibular disorders, etc.) Also, why did you choose the mBESS balance scoring system compared to other tests? Are there other tests that could have been utilized?
LikeLike
Hey folks, I was wondering if foot size (length/width) is something worth controlling for in subjects considering it may provide an anatomical benefit. Is that something that has been researched previously?
LikeLike
Thanks for the questions Faye and Erik.
Faye-
With excluding those personal characteristics from the study, we attempted to eliminate any conditions or injuries that may have affected balance. We chose the mBESS due to its ability to measure static balance. It was very efficient and easy to score with the number of participants in a short amount of time. It also has good reliability. There are other measures of balance that we could have used, an example being the Y-Balance task which measures dynamic balance. There are comments above that speak on the Y-Balance specifically. Great questions.
Erik – I’m happy you brought up foot size and how it may affect balance. In one instance, having large feet did contribute to perfect balance, but I would consider it anecdotal evidence. There were also those with small feet who scored great on the mBESS. A person with average height with a shoe size 12, may have better balance than Shaquille O’Neal with a size 12. The size of the foot would be relative to their height. It would be interesting to see how people score who have larger feet compared to their height. There was no previous research found on this topic specifically during our literature review.
LikeLike