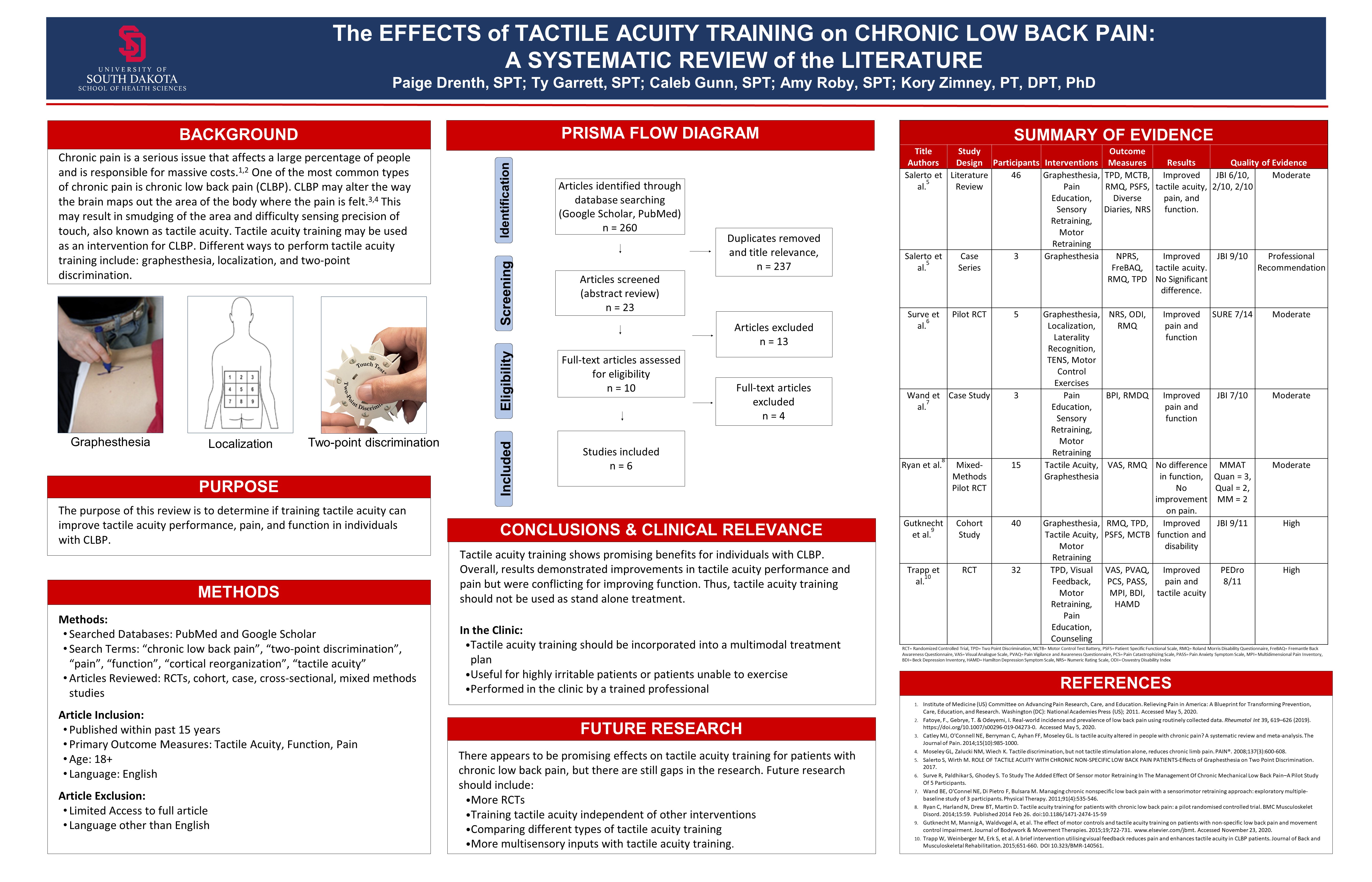
The Effects of Tactile Acuity Training on Chronic Low Back Pain: A Systematic Review of the Literature
Click on image to expand
Paige Drenth, SPT, Ty Garrett, SPT, Caleb Gunn, SPT, Amy Roby, SPT
Click on image to expand
Paige Drenth, SPT, Ty Garrett, SPT, Caleb Gunn, SPT, Amy Roby, SPT

Question: I notice that tactile acuity training proposed beneficial results for tactile acuity performance and pain but not for function (conflicting). Was there a specific reason for a lack of improvement in function (as one would think there could be improved ability following a decrease in pain symptoms)?
Question: I see your inclusion criteria includes individuals aged 18 years and older. Did you find tactile acuity training to be more beneficial for a more specific age group/gender versus another?
LikeLike
Great questions Tiegen! We believe that the lack of improvements with function was due to tactile acuity training largely targeting sensory inputs. Motor function is a large multidimensional system that includes many different aspects such as strength, balance, proprioception, mobility, etc. Thus, tactile acuity is just a small component within that large multidimensional system which could have contributed to the lack of improvement. For your second question, unfortunately none of the studies included investigated if tactile acuity was more beneficial for specific age groups or gender. That would definitely be an interesting topic for future research!
LikeLike
Did any of the studies included in your systematic review discuss patient education on the purpose behind tactile acuity training for CLBP or were there any difficulties with establishing patient buy-in?
LikeLike
Great question Rachael! Some of the studies did include patient education. Before treatments began, they held education sessions to discuss the complexity of pain, how pain can correlate with poor body perception (tactile acuity), and how tactile acuity training can potentially help. Some of the studies did not state anything about patient education on pain or tactile acuity. Lastly, one of the studies included an interview with the subjects post-intervention to discuss their perceptions of the treatments. Some people felt that the tactile acuity training took too long or was annoying. Another participant stated that it was difficult because lying on their back for extended periods was very uncomfortable. I definitely think there could be difficulties with patient buy-in. Addressing barriers and providing quality education would be very important if offering tactile acuity training as a treatment.
LikeLike
Great job guys! I found the information presented in this poster interesting and very informative. In the research, did you notice if one intervention in specific was more successful than other interventions? In the conclusions, you stated that it should not be used as a stand-alone treatment, what other interventions would you recommend to use with tactile acuity? Thanks!
LikeLike
Tactile acuity training is best used within a treatment approach that combines different strategies. There was not one intervention to be found to be superior than another. Current evidence suggests that a combination of tactile acuity, manipulations or mobilizations, and exercise helps decrease pain and improve function. Activities such as motor control, resistance, or aerobic exercise have been utilized and found to be beneficial.
LikeLike
Pain neuroscience education and somatosensory training techniques such as tactile acuity are interesting intervention strategies that, as you show here, have promising beneficial effects for chronic pain patients. It’s evident that the best outcomes are when it is combined with other movement interventions. I was wondering if you came across any research, or what your opinion is, on how tactile acuity training compares to other widely used pain relief methods, such as soft tissue mobilization or heat and e-stim, when incorporated with exercise programs?
LikeLike
Great question Drew! None of our articles specifically looked at adding tactile acuity with other modalities or compared their effectiveness with other modalities. I would say that there are some similarities between tactile acuity training with other modalities in the fact that we are applying a sensory input in order to recondition different aspects of the brain. I would say the main difference between tactile acuity training and different modalities are the fact that tactile acuity training is an active process where an individual has to cognitively think about the sensory input being applied instead of passively sitting there with a sensory input being applied. It would be nice to have different studies to look at this comparison though!
LikeLike
Great poster everyone! Question regarding conclusions made – Can you further explain why you state there’s conflicting evidence for improved function when most articles show ‘moderate’ (and one ‘high’) evidence for improved function? I think this is great research and an interesting topic. I can’t wait to follow along with some of the other questions being asked! 🙂
LikeLike
Great question Kristi! Although there were multiple studies that showed improvement with certain self-reported indexes in regards to function, there were also multiple studies that showed no improvements with self-reported indexes in regards to function. Due to the limited research on this current topic as well as the narrow margin between the results of each article, we did not feel comfortable labeling improvement’s in function as significant. We believe that there is the potential with future research to demonstrate this, but there was enough conflicting evidence that we had to label improvements in function as conflicting at this moment. Our group hypothesized that improvements in function can incorporate more motor pathways and various components that may or may not be targeted with a more sensory dominated form of treatment. Great question and thank you for asking!
LikeLike
At a continuing education course I attended recently, they categorized low back pain into three different categories: movement disorders with no neurological symptoms, lumbar spine pain with instability, and lumbar spine pain with radicular pain. In your research, did you come across any evidence that tactile acuity benefits one type of chronic LBP as opposed to other causes of LBP. From a pain neuroscience education stand point, do you think this treatment intervention would reduce nociceptive, neuropathic, or nociplastic pain the most based on the science behind this intervention.
LikeLike
Great questions! In terms of categorizing which group that tactile acuity training would best serve I am unable to really foresee tactile acuity benefitting one of those groups over any other. From what I understood of the research, tactile acuity would be best suited for conditions that have little to no tissue or structural damage but rather the brain’s own perception of pain from different sensory receptions throughout the lower back. Tactile acuity training, in my opinion, would maybe best be compared to intervention treatments such as phantom pain syndrome in which there is no structural damage. The body understands there is pathological tissue there but the brain has an altered perception of the area. I would still recommend other forms of treatments with potential addition of tactile acuity training with other low back pain conditions that need to add various components of stability or mobility, but tactile acuity training is more used to retrain the brain rather than retrain the low back in my opinion.
I would consider tactile acuity training as an intervention treatment best aimed at nociceptive pain conditions. We are essentially trying to retrain the brain in specific terms from either hyperalgesia conditions or allodynia conditions in which their is an internal miscommunication issue. Great questions!
LikeLike
I thought that your poster was very informative and I learned a lot! When reviewing the information, I was curious what the average age was of the participants in your systematic review. You also stated that chronic low back pain can alter the brain map resulting in smudging. Do you think that other interventions that aim to help with cortical remapping such as graded motor imagery or laterality testing could improve tactile acuity as well?
LikeLike
Great questions Whitney! The average age of the participants varied quite a bit. Some of the studies looked at people as young as 18-20 and as old 65-66, which a good mixture of ages between. Laterality training could potentially be helpful because cortical remapping can affect someone’s laterality judgement. I think graded motor imagery can potentially be beneficial as well because, theoretically, it helps retrain the brain to not think of certain movements as being harmful. Some of the studies included laterality training and graded motor imagery, which definitely could contribute to positive results. As with tactile acuity training, however, further research probably needs to be conducted for these before we can really say for sure.
LikeLike
Tactile acuity training is an interesting intervention technique that was unfamiliar to me prior to my second year in the PT program. I thought you all did a great job covering the topic. When reviewing the information presented in the poster I became curious about at home tactile acuity training. I read in an article that one main barrier in tactile training was the application of the intervention outside of the clinic, without a PT to apply the technique. Did your research group find any supporting information discussing how tactile acuity training is modified for patients who are asked to complete these interventions outside of the clinic?
LikeLike
Thanks for the question Dayton! One of the studies we analyzed included tactile acuity training as a home program. In this study, the researchers gave each participant a DVD that demonstrated the technique and a simple instruction manual. Unfortunately the researchers did not find success with the tactile acuity home program. The researchers found many barriers with the home program such as lack of time, lack of understanding of intervention, and not having another person to administer the intervention. We believe that a home tactile acuity program could be effective but it would require proper training of the person administering the intervention and the patient must be committed to following the home program. Future research looking at ways to better administer home tactile acuity training is definitely warranted.
LikeLike
Great job with your presentation! I noticed in your poster that some of the studies used resulted in improved pain, function, and tactile acuity while others resulted in no difference/no improvement in function or pain. Can you explain the methods of each of these conflicting studies? Perhaps the dosing of the tacitly acuity intervention or participant recruitment method differences of these studies may help me to understand the conflicting results. Thank you!
LikeLike
When comparing the results of each of the studies the authors reported different outcomes relating to function (ie PSFS, RMDQ, and the ODI). We covered different types of study designs such as: literature reviews, randomized controlled trials, and case series. The delivery of tactile acuity (whether it was graphesthesia or two-point discrimination), co-interventions, inclusion of pain education, and the use of visual feedback were main contributors to what we viewed as the differences for improvement in functional outcomes versus not. The study by Gutknecht et al. compared their data to historical data which may attribute to differences in PSFS and RMDQ scores. There were also large between group differences at baseline when for measuring PSFS scores which may have caused there to be no overall significant changes. Each of the studies included a varied number of participants and recruitment strategies. An experimental study we included by Surve et al. found significant improvements, however had a 10 week strategy for implementing multiple types of tactile stimulus and motor control interventions. Another difference we found was the motor training that was provided. Ryan et al created a pilot RCT and found no improvement in function. However, we attributed this to the delivery method of the tactile acuity training and not necessarily recruitment or dosing. I hope this helps!
LikeLike