Pregnancy was included as an exclusionary criteria due to possible presence of gestational diabetes and changes in sensory, especially tactile, stimuli interpretation.
Leonard- great question. Macey is spot on with her answer as to the physiological phenomena that occurs with pregnancy. Our study was to be of healthy individuals who were, for the most part, homogeneous. We find that most studies exclude pregnancy from their list due to the changes that Macey described- if we have twenty individuals in a study and a few are pregnant, the few pregnant subjects could potentially skew the data- thus giving us a result that would not be applicable to the population at large. I recall a pharmacology professor of ours describing how pregnancy is listed as a warning or no-use for some medications is due to the fact that no studies have been published studying the effects of a treatment/medication on the woman or child. We excluded pregnancy to keep our data from being skewed- however, future studies could focus on this population and see if they compare to healthy, non-pregnant populations.
Great study, colleagues. I’m curious what your thoughts are regarding why the hand demonstrated poor reliability with descending and randomization testing. Correct me, but doesn’t the hand have greater sensory feedback than the other testing sites? I would have assumed that despite randomization the hand should yield better reliability. Thanks!
Katie, good question. Yes, you are correct that the hand has the highest tactile acuity out of the three testing locations. It is hard to say exactly why the hand had poor reliability for the descending with randomization and two-point estimation methods, as it could be related to any of our limitations. In addition to having the best overall reliability, the ascending-descending method also had the lowest minimal detectable difference for all three testing sites compared to the other two methods, which is important to determine if a true change in TPD has occurred when checking progress with your patients. It is was also interesting that the hand did have the smallest minimal detectable difference for all three testing methods, compared to the other two testing sites. There may also be a potential floor effect with the smaller measurements at the hand.
Nice Job! Just a few questions: Were the participants informed of the descending and ascending methods? Whether they were or not, were the procedures conducted in the descending –> ascending –> ‘descending with randomization’ order for each participant at each location or was the testing order randomized? Thanks!
Great question Austin!
Participants were not informed if the caliper was ascending or descending, meaning wether the distance between the two points would be increasing or decreasing. During the randomization method, participants were again not told that researchers would be alternating between one and two points in order to find their TPD threshold. The consist line told to participants was that they would be touched with the caliper and that participants should report one if one point was felt and two if two points were felt. As far as order of testing, this too was held consistent for all participants. Descending-ascending method was performed first at all three locations, then descending with randomization at all three locations, then two-point estimation again at all three locations. This sequence was then repeated by the second researcher in the same manner.
I hope this answers your questions!
Hey guys! Just a few questions about your study that I’m curious about, and maybe it doesn’t matter but I’m gonna ask anyway. Did you guys standardize the positioning of the subjects (i.e. sitting, laying, standing)? Please explain which position if you did and whether positioning can impact TPD. Additionally, I know you touched on this in your oral presentation but can you remind me why a limitation of the study is exercise prior to testing?
We had each individual sit in a standard chair without arm rests while placing their dominant side foot on a chair placed in front of them- they remained in this position for the entirety of the three testing methods. We did this based upon patient comfort- previous studies have had patients in various positions such as seated, prone, or long sitting. Most of these studies only looked at specific regions (back only, UE only, LE only, etc). As we were testing UE, LE, and upper trap, we needed a position that would minimize movement out of the subject while still allowing access to the test sites. As of now, we are unsure if position can impact TPD values- but this would be a good future idea for a research study!
As far as exercise is concerned- we noticed that individuals who came in immediate post-exercise tended to have an increased erythema response to the points being placed to the skin. This makes sense if we think about the physiology of exercise- increased blood flow to the skin and muscles. If we follow pain neuro principles that nerves like space, movement, and BLOOD then we may see a difference in peripheral nerve sensitivity immediate post-exercise due to increased peripheral blood flow. I believe that a study on the effect of exercise on TPD would be very interesting.
Gina, Macey, Jordan- nice work! Interesting study! I’m wondering what you three think are some of the clinical implications are for having poor discrimination estimation? These were seemingly healthy individuals- do you three think this poor discrimination estimation is important? It appears to be important in people with chronic regional pain syndrome – however, this study suggests that even healthy individuals may struggle with it.
Stephanie,
The poor results at the two locations with the two-point estimation method indicate the testing reliability is poor between two clinicians testing the same locations with the same method. Therefore, the two-point estimation method would not be a good, reliable method to use at the upper trap or hand if a patient had one clinician test his TPD one day and another clinician test his TPD another day. We would advise clinicians to use a more reliable TPD method for those locations if different clinicians were testing the same patient. Yes, knowing the two-point estimation method had poor inter-rater reliability results at the upper trap and hand are important as it tells us this is not a good method to use in the clinic if a clinician wants reliable TPD results between two clinicians. From our study, we can only say the two-point estimation method is not the best method to use in the clinic for the upper trap or hand based off inter-rater reliability; we can’t assume for our study that the individual is struggling with TPD as it could be just the method. It would be interesting to look more into TPD results comparing healthy individuals and individuals with chronic regional pain syndrome.
Stephanie-
I agree that the healthy participants used in this study had a difficult time during testing at points and therefore could be confusing as to when to use this testing method in clinic. To classify TPD as important or non-important is difficult as each situation is different with multiple different factors. I think you bring up a great patient population in complex regional pain syndrome. TPD falls under the category of graded motor imagery, which has been shown as useful and effective treatment methods with these patients. I personally believe that TPD could be useful in patients where other objective measurements involving movement and activity are too strenuous or when subjective reporting has been inconsistent. A patient’s TPD threshold could be used as a method to track patient progress through therapy, with smaller thresholds indicating better outcomes. Therapists would have to keep in mind that normative values for TPD have not been established and validated in
literature to my knowledge, so in essence there would not be a magical threshold number to shoot for during therapy. TPD may not be as appropriate or informative in all patients, however, it can still provide useful information into the state of the patient’s sensory interpretation with implications on their cortical organization, which can also be implicated in the pain they are experiencing.
Great research guys! Sorry for the late question. Lots of good questions have been addressed and answered. Where do you guys see this research going in the future? And what would you guys do differently for next time?
Colton- we would love to see future research that focuses on the effects of exercise on TPD values. Further, we were astonished to find that there is no current research comparing dominant vs. non-dominant limbs during our literature review. We would like to see future research focus on these differences or lack thereof. Since we usually compare our injured limb to that of the non-involved limb, it would be important to make sure that there are no significant differences between both healthy limbs prior to using TPD.
Hello all, great poster presentation! Sorry for the late post, I just have a couple quick questions. First, what was the reasoning behind the testing site choices? Also, do you believe that reporting the values out loud during testing could have led to bias? When I participated in the study I had no clue what the numbers meant, so I am just curious! Thanks for the hard work guys, very interesting study.
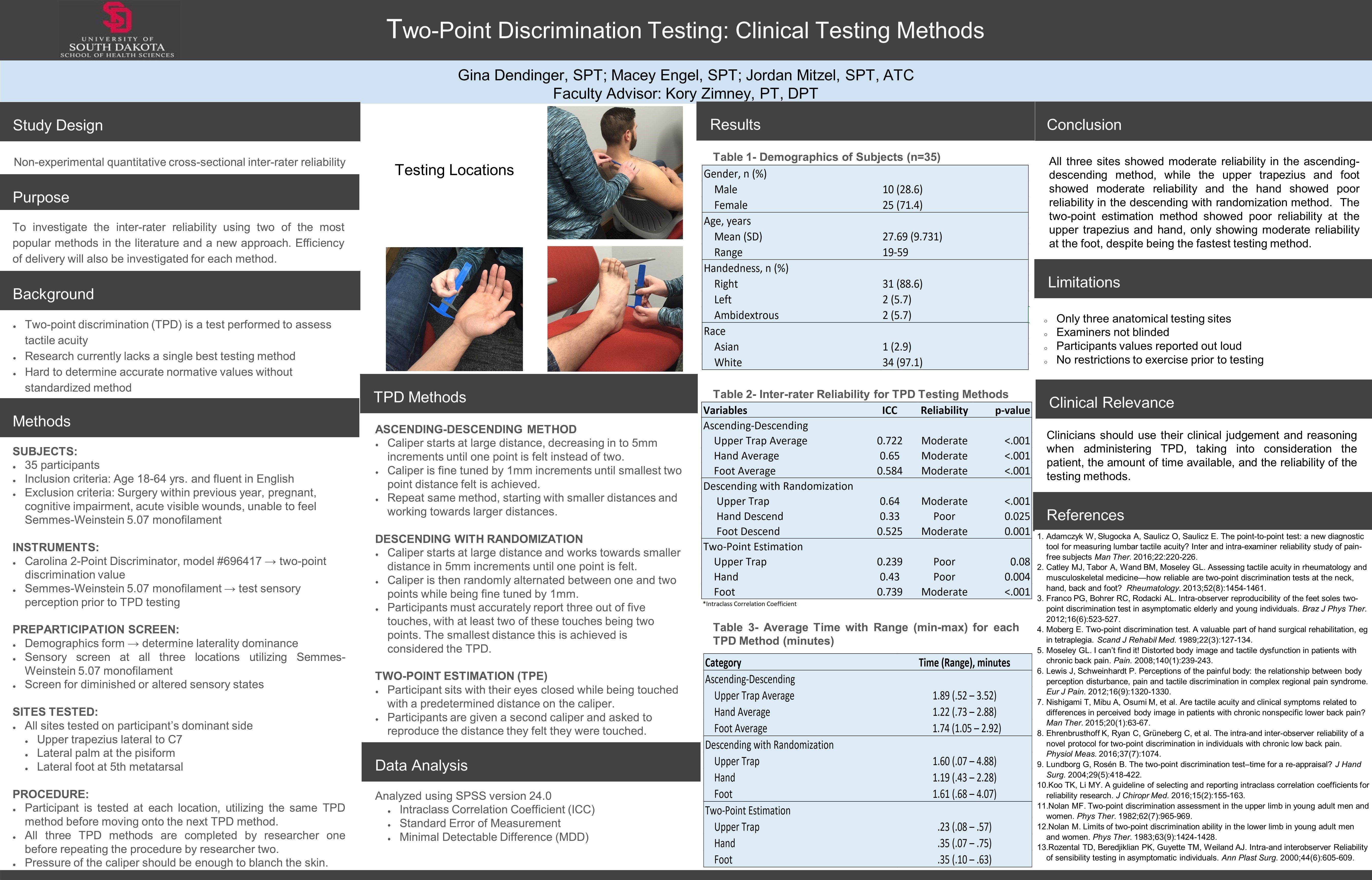
There were a few reasons why we chose the three sites we did. First, these sites had already been previously tested by other researchers, giving us values that we could compare our results to. Second, these sites are common sites of chronic pain issue- the upper trap during whiplash mechanisms, and the hand and foot due to crush/CRPS. Lastly, these sites were easy to access and were able to be easily found consistently due to the nearby bony landmark allowing guidance for the testing technique.
We are not not sure if our announcing the TPD values out loud affected the study at all, however, we did list it as one of our limitations and if we were able to go back and re-do the study, we agreed that we would not announce them out loud, but rather just show the value to the recorder.

This is an interesting study. Can you please explain why pregnancy is exclusionary? Thank you for your work on this!
LikeLike
Pregnancy was included as an exclusionary criteria due to possible presence of gestational diabetes and changes in sensory, especially tactile, stimuli interpretation.
LikeLike
Leonard- great question. Macey is spot on with her answer as to the physiological phenomena that occurs with pregnancy. Our study was to be of healthy individuals who were, for the most part, homogeneous. We find that most studies exclude pregnancy from their list due to the changes that Macey described- if we have twenty individuals in a study and a few are pregnant, the few pregnant subjects could potentially skew the data- thus giving us a result that would not be applicable to the population at large. I recall a pharmacology professor of ours describing how pregnancy is listed as a warning or no-use for some medications is due to the fact that no studies have been published studying the effects of a treatment/medication on the woman or child. We excluded pregnancy to keep our data from being skewed- however, future studies could focus on this population and see if they compare to healthy, non-pregnant populations.
LikeLike
Great study, colleagues. I’m curious what your thoughts are regarding why the hand demonstrated poor reliability with descending and randomization testing. Correct me, but doesn’t the hand have greater sensory feedback than the other testing sites? I would have assumed that despite randomization the hand should yield better reliability. Thanks!
LikeLike
Katie, good question. Yes, you are correct that the hand has the highest tactile acuity out of the three testing locations. It is hard to say exactly why the hand had poor reliability for the descending with randomization and two-point estimation methods, as it could be related to any of our limitations. In addition to having the best overall reliability, the ascending-descending method also had the lowest minimal detectable difference for all three testing sites compared to the other two methods, which is important to determine if a true change in TPD has occurred when checking progress with your patients. It is was also interesting that the hand did have the smallest minimal detectable difference for all three testing methods, compared to the other two testing sites. There may also be a potential floor effect with the smaller measurements at the hand.
LikeLike
Nice Job! Just a few questions: Were the participants informed of the descending and ascending methods? Whether they were or not, were the procedures conducted in the descending –> ascending –> ‘descending with randomization’ order for each participant at each location or was the testing order randomized? Thanks!
LikeLike
Great question Austin!
Participants were not informed if the caliper was ascending or descending, meaning wether the distance between the two points would be increasing or decreasing. During the randomization method, participants were again not told that researchers would be alternating between one and two points in order to find their TPD threshold. The consist line told to participants was that they would be touched with the caliper and that participants should report one if one point was felt and two if two points were felt. As far as order of testing, this too was held consistent for all participants. Descending-ascending method was performed first at all three locations, then descending with randomization at all three locations, then two-point estimation again at all three locations. This sequence was then repeated by the second researcher in the same manner.
I hope this answers your questions!
LikeLike
Hey guys! Just a few questions about your study that I’m curious about, and maybe it doesn’t matter but I’m gonna ask anyway. Did you guys standardize the positioning of the subjects (i.e. sitting, laying, standing)? Please explain which position if you did and whether positioning can impact TPD. Additionally, I know you touched on this in your oral presentation but can you remind me why a limitation of the study is exercise prior to testing?
LikeLike
Dusty,
We had each individual sit in a standard chair without arm rests while placing their dominant side foot on a chair placed in front of them- they remained in this position for the entirety of the three testing methods. We did this based upon patient comfort- previous studies have had patients in various positions such as seated, prone, or long sitting. Most of these studies only looked at specific regions (back only, UE only, LE only, etc). As we were testing UE, LE, and upper trap, we needed a position that would minimize movement out of the subject while still allowing access to the test sites. As of now, we are unsure if position can impact TPD values- but this would be a good future idea for a research study!
As far as exercise is concerned- we noticed that individuals who came in immediate post-exercise tended to have an increased erythema response to the points being placed to the skin. This makes sense if we think about the physiology of exercise- increased blood flow to the skin and muscles. If we follow pain neuro principles that nerves like space, movement, and BLOOD then we may see a difference in peripheral nerve sensitivity immediate post-exercise due to increased peripheral blood flow. I believe that a study on the effect of exercise on TPD would be very interesting.
LikeLike
Gina, Macey, Jordan- nice work! Interesting study! I’m wondering what you three think are some of the clinical implications are for having poor discrimination estimation? These were seemingly healthy individuals- do you three think this poor discrimination estimation is important? It appears to be important in people with chronic regional pain syndrome – however, this study suggests that even healthy individuals may struggle with it.
LikeLike
Stephanie,
The poor results at the two locations with the two-point estimation method indicate the testing reliability is poor between two clinicians testing the same locations with the same method. Therefore, the two-point estimation method would not be a good, reliable method to use at the upper trap or hand if a patient had one clinician test his TPD one day and another clinician test his TPD another day. We would advise clinicians to use a more reliable TPD method for those locations if different clinicians were testing the same patient. Yes, knowing the two-point estimation method had poor inter-rater reliability results at the upper trap and hand are important as it tells us this is not a good method to use in the clinic if a clinician wants reliable TPD results between two clinicians. From our study, we can only say the two-point estimation method is not the best method to use in the clinic for the upper trap or hand based off inter-rater reliability; we can’t assume for our study that the individual is struggling with TPD as it could be just the method. It would be interesting to look more into TPD results comparing healthy individuals and individuals with chronic regional pain syndrome.
LikeLike
Stephanie-
I agree that the healthy participants used in this study had a difficult time during testing at points and therefore could be confusing as to when to use this testing method in clinic. To classify TPD as important or non-important is difficult as each situation is different with multiple different factors. I think you bring up a great patient population in complex regional pain syndrome. TPD falls under the category of graded motor imagery, which has been shown as useful and effective treatment methods with these patients. I personally believe that TPD could be useful in patients where other objective measurements involving movement and activity are too strenuous or when subjective reporting has been inconsistent. A patient’s TPD threshold could be used as a method to track patient progress through therapy, with smaller thresholds indicating better outcomes. Therapists would have to keep in mind that normative values for TPD have not been established and validated in
literature to my knowledge, so in essence there would not be a magical threshold number to shoot for during therapy. TPD may not be as appropriate or informative in all patients, however, it can still provide useful information into the state of the patient’s sensory interpretation with implications on their cortical organization, which can also be implicated in the pain they are experiencing.
LikeLike
Great research guys! Sorry for the late question. Lots of good questions have been addressed and answered. Where do you guys see this research going in the future? And what would you guys do differently for next time?
Thanks.
LikeLike
Colton- we would love to see future research that focuses on the effects of exercise on TPD values. Further, we were astonished to find that there is no current research comparing dominant vs. non-dominant limbs during our literature review. We would like to see future research focus on these differences or lack thereof. Since we usually compare our injured limb to that of the non-involved limb, it would be important to make sure that there are no significant differences between both healthy limbs prior to using TPD.
LikeLike
Hello all, great poster presentation! Sorry for the late post, I just have a couple quick questions. First, what was the reasoning behind the testing site choices? Also, do you believe that reporting the values out loud during testing could have led to bias? When I participated in the study I had no clue what the numbers meant, so I am just curious! Thanks for the hard work guys, very interesting study.
LikeLike
There were a few reasons why we chose the three sites we did. First, these sites had already been previously tested by other researchers, giving us values that we could compare our results to. Second, these sites are common sites of chronic pain issue- the upper trap during whiplash mechanisms, and the hand and foot due to crush/CRPS. Lastly, these sites were easy to access and were able to be easily found consistently due to the nearby bony landmark allowing guidance for the testing technique.
We are not not sure if our announcing the TPD values out loud affected the study at all, however, we did list it as one of our limitations and if we were able to go back and re-do the study, we agreed that we would not announce them out loud, but rather just show the value to the recorder.
LikeLike