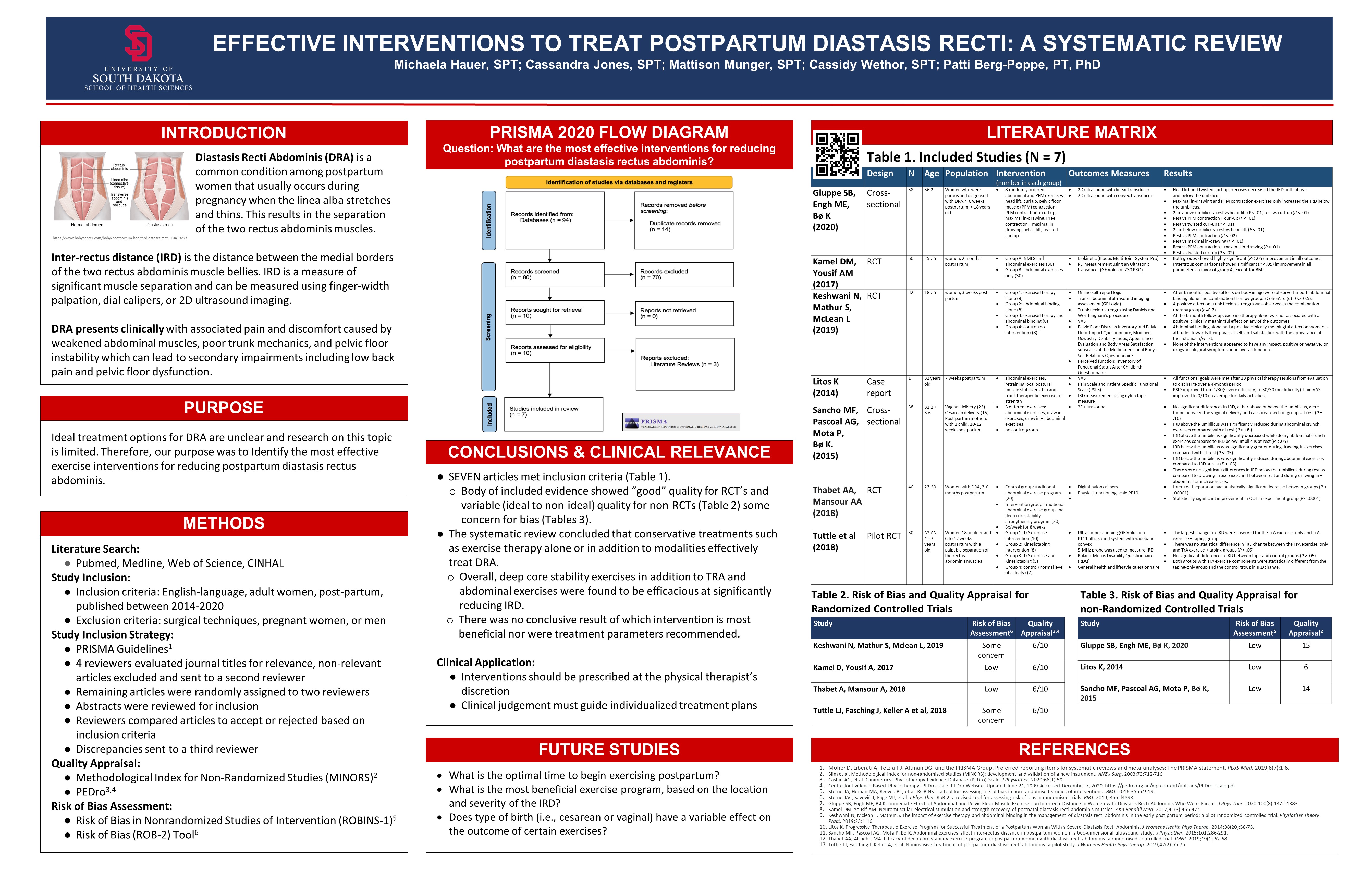
Effective Interventions to Treat Postpartum Diastasis Recti: A Systematic Review
Click on image to expand
Michaela Hauer, SPT, Cassandra Jones, SPT, Mattison Munger, SPT, Cassidy Wethor, SPT
Click on image to expand
Michaela Hauer, SPT, Cassandra Jones, SPT, Mattison Munger, SPT, Cassidy Wethor, SPT

Was there any research regarding exercise during pregnancy and if that altered the likelihood of experiencing diastasis recti? If so, what kind of exercises were recommended or not recommended?
LikeLike
Jessica: For our research, we excluded antenatal conservative management of diastasis recti abdominis (DRA) and mainly focused on postnatal management. However, according to the research, non-specific exercise can reduce the risk or presence of DRA in antenatal and postnatal women. In addition to non-specific exercise, best-evidence also recommends exercises that target abdominal muscles to reduce the risk or presence of DRA in pregnant women. Exercises include pelvic tilts, transverse abdominis muscle control, pelvic floor exercises, and functional exercises with emphasis on transverse abdominis contraction. With all of these exercises, it is important to teach proper technique to avoid excess pressure in the abdomen as well as bulging of the abdominal muscles. Based on these results, it is recommended to assess antenatal and postnatal women for DRA and recommend best-evidence exercise to improve quality of life in these populations.
LikeLike
Very nice poster, guys. During your research, did you come across any risk factors or specific variables that makes one more susceptible to DRA (outside of pregnancy)? Additionally, did you happen to see a trend in the approximate amount of time it took to reduce IRD with exercise? Thanks!
LikeLike
Trey: Our research found other risk factors that make one more susceptible to DRA include abdominal obesity, considerable weight loss in a short amount of time, diseases that affect the production of collagen, persistent cough from smoking, and poor/improper form during exercise. Risk factors during pregnancy that increase one’s risk of DRA include multiple pregnancies, a short interval of time between pregnancies, age greater than 35, high birth weight, high volumes of amniotic fluid, weight gain during pregnancy, and physical activity before and during pregnancy.
Majority of studies included in this systematic review concluded after 8 weeks, all with reductions in IRD with exercise. Clinically, I would suggest treatment for 6-8 weeks as this is the typical amount of time it takes to build strength. However, one study did have significant reduction in IRD after two weeks which shows how important it is to provide patient centered care based on patient progression and presentation of impairments.
LikeLike
Thank you for providing this information on postpartum diastasis recti and the current best available interventions to reduce its impact. This diagnosis and its effects was novel to me, so I appreciated learning about it through your research.
I noticed that the study by Keshwani, Mathur, and McLean (2019) noted positive effects on body image that were observed through interventions. I thought this finding was intriguing, for I know from conversations with friends that postpartum body image can be a real struggle for some women. I think it is important we are considering the mental and emotional health of our patients as well, and this may be a unique consideration for this population of patients. I know your main research question was looking at exercise interventions, but did you find that any of the other included studies mentioned body image or examined it through an outcome measure? Do you have any thoughts regarding this topic and whether it would be important or not to assess in these patients?
Thank you!
LikeLike
Maddison: Thank you for your questions. Unfortunately, none of the other included studies provided outcome measures to compare body image before and after interventions or even mentioned body image. Body image can have a large impact on the mental health of postpartum women. We think that future studies focusing on postpartum women and interventions that could improve body image and contribute to a positive improvement in mental health would be beneficial for future clinicians and help them be more aware of how to further help their postpartum population.
LikeLike
Great job with your research! In your introduction of DRA, you mentioned that IRD is a significant measurement of the separation of the two muscle bellies. In your research, did you come across different categories of DRA based on the IRD? For example, what is considered a significant separation compared to a moderate or minimal separation of the two muscle bellies? Do you think interventions should be prescribed differently based on IRD?
LikeLike
A DRA is considered pathologic when the interrecti distance (IRD) measurement exceeds 2.5 to 2.7 cm width and severity ranges from mild (2.5-3.4 cm) to severe (5-20 cm or greater). The studies we utilized in our systematic review used different methods to measure this distance such as the finger width measurement, nylon calipers, or a 2D ultrasound machine. If the separation is greater than 2 finger widths, it is considered DRA. In my opinion, patients who present with a distance greater than 2 cm would need extra time and adherence to the exercise program to close the gap as opposed to patients who have a smaller separation distance. For example in the case study we utilized, the patient had an 11.5 cm separation and was able to significantly reduce the distance to 2.0 cm using abdominal and other strengthening techniques over a 4 month period. Patients with large interrectus distances or do not respond to physical therapy could be candidates for surgery. I think transversus abdominis/core, abdominal, and pelvic floor strengthening would be appropriate for most patients regardless of DRA distance. However, it is important to give each patient a plan of care that is tailored to their needs and impairments.
LikeLike
Good job everyone! Do you know if any studies found a correlation between the initial size of the IRD and how well that person would respond to the interventions? For example, if someone with a larger initial IRD did not respond as well to treatment as someone with a smaller IRD.
LikeLike
For these studies, the criteria to be a participant was to have at least 2 finger widths (2.5 cm) or greater of a distance between the rectus abdominis muscles. The studies did not provide individual measurements for each of the participants. In the case study we utilized, the patient had an 11.5 cm separation and was able to significantly reduce the distance to 2.0 cm using abdominal and other strengthening techniques over a 4 month period. This leads me to believe that while patients with a smaller interrectus distance would have better outcomes, it is also possible for patients with severe DRA to have successful outcomes from conservative treatment.
LikeLike
Very well put together poster everyone! Did any of the studies talk about things that could be done prophylactically for DRA? Trey asked you guys about risk factors associated with DRA. If people present with these risk factors, is there anything we can do before the pregnancy to help lower the severity of IRD?
LikeLike
Bailey: Things that can be done prophylactically to prevent DRA or the severity of it include proper core activation mechanics, nutrition, daily or consistent exercise routine antenatal and during pregnancy, and targeted abdominal exercise for people with a known increased IRD pre-pregnancy.
LikeLike
Nice work guys! In your introduction, you mentioned some other conditions that can occur along with DRA such as LBP and pelvic floor dysfunction. Did any of the studies involve these conditions as well, and if so, how?
LikeLike
Austin: Some of the studies did include secondary outcome measures that focused on the effect of the included interventions for low back pain and pelvic floor dysfunction and were measured by various tools. There have also been other studies that have suggested that strengthening the TRA will help to alleviate symptoms of low back pain and pelvic floor dysfunction. Therefore, the interventions included in these studies could be beneficial to physical therapists who are treating postpartum low back pain and pelvic floor dysfunction such as urinary incontinence.
LikeLike
Great job with the presentation. I know it was mentioned there was no preferred intervention, but do you think there is a most efficient treatment plan to treat this? For the abdominal exercises, did you find a repetition range for the exercises that will maximize the benefits? Or if isometrics, concentric, or eccentrics exercises are better?
LikeLike
Justin: A majority of our studies had great results with standard abdominal exercises including an abdominal crunch, twisted curl-up, and deep core activation. The most important part of these exercises is to ensure proper core activation without valsalva or compensations. Most of the studies prescribed a range of 12-15 repetitions and had great success. This range helps to improve endurance and motor control of the musculature which has been impaired due to the separation. None of the studies highlighted concentric or eccentric to be better than the other, however isometrics have been shown to be successful at reducing pain in other muscle groups so it is likely a better option for someone experiencing abdominal pain.
LikeLike
Great presentation and poster everyone! I know that it was noted that no specific parameters were recommended through the research, but I was wondering what parameters you would possibly use with patients with DRA after reading through the research? I am just curious if there were any patterns throughout different studies on the sets, repetitions, ect. that were used with the patients in the studies.
LikeLike
Emily: Depending on where a patient may be postpartum, the sets, repetitions, and difficulty of targeted abdominal exercises will be different. Typically, we saw that most studies preferred 2-3 sets per exercise and repetitions varied from 8-20. The most common number of repetitions being 12-15 to target muscle endurance. These are similar parameters that we would use after reading the research. Personal factors that we would take into account when creating a plan of care would be proper technique, healing, and patient tolerance as some patients may not tolerate high repetitions in the beginning.
LikeLike
Great job with your poster! I noticed in Table 1 that only a few studies specified that the women recruited in the study were parous. Did some of your studies include nulliparous women as well? If so, did you find any information on the correlation between women who have given birth multiple times and their IRD compared to women who have only given birth once?
LikeLike
Rachel: Most of our studies included women who were primiparous or multiparous. The studies didn’t give specific details on outcomes based on parity in the participants. However, being multiparous or pluriparous are risk factors for DRA so it could be hypothesized that the amount of children birthed and IRD distance/DRA would be positively correlated, especially if DRA wasn’t corrected before becoming pregnant again. This is a great question and is an ideal topic for future research.
LikeLike
Great poster and what an interesting topic. I understand your research question regarded interventions for DRA, however did you find any correlation between DRA , Interventions, and they type of birth each individual underwent? I see you listed that in ‘future research’, but was curious if you found anything while researching?
LikeLike