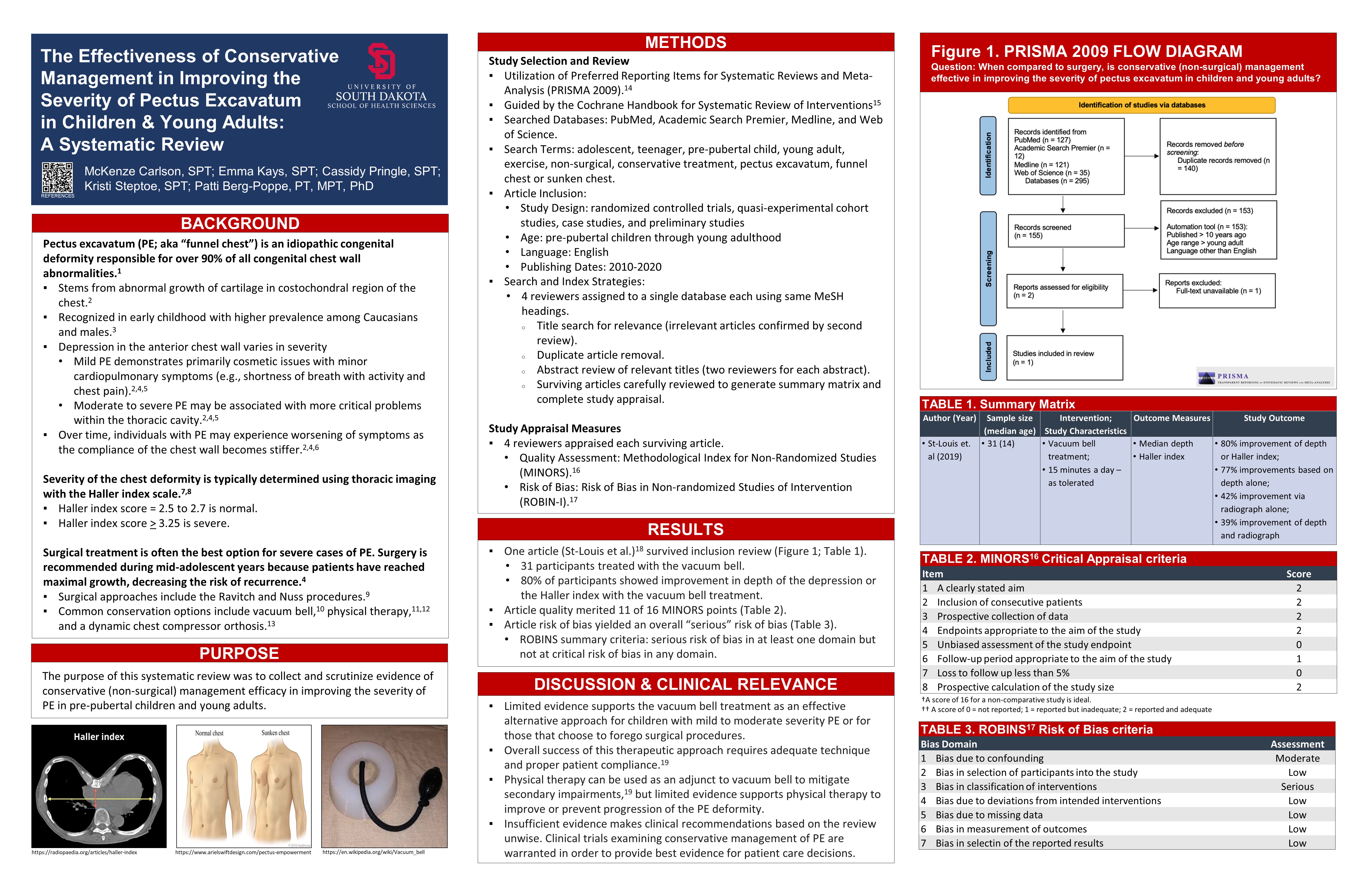
The Effectiveness of Conservative Management in Improving the Severity of Pectus Excavatum in Children & Young Adults: A Systematic Review
Click on image to expand
McKenze Carlson, SPT, Emma Kays, SPT, Cassidy Pringle, SPT, Kristi Steptoe, SPT
Click on image to expand
McKenze Carlson, SPT, Emma Kays, SPT, Cassidy Pringle, SPT, Kristi Steptoe, SPT

In your article that you reviewed, did the authors discuss what type of physical therapy interventions were used? If not, what are some ideas for some PT interventions that you may utilize?
LikeLike
Thanks for the question Tristen. Unfortunately the article review did not discuss physical therapy interventions – just the vacuum bell treatment. However, we did come across a case report early on in our literature search that provided insight into what PT could look like with patients with a chest wall deformity such as pectus excavatum. When you look at kids with pectus excavatum, it’s not just a cosmetic defect, it can affect the cardiopulmonary system, musculoskeletal system, and even neuromuscular system (and so much more). So working on breathing techniques (diaphragmatic breathing, box breathing, etc.), thoracic spine and rib cage mobilizations, strengthen paraspinal and parascapualar musculature are all great places to start.
LikeLike
Regarding future research on the conservative management of pectus excavatum, did any of the articles offer insight on what clinical trials or further research may include?
LikeLike
Thanks for the question Jessica. Since there was only one article that we were able to find based our inclusion and exclusion criteria, future research might just include more research, or a larger sample sizes regarding the effectiveness of the vacuum bell treatment, since it is so limited. As a group, we would love to see future research on the effects of physical therapy alone on children with PE or even the effects of PT in addition to the vacuum bell treatment on children with PE! More research is also needed on the appropriate time to implement conservative options.
LikeLike
Did the efficacy of the conservative management differ at all based on the age? Did younger individuals have any supporting evidence that could potentially improve their situation or even reduce the overall impact of the condition compared to older children or potentially teens?
LikeLike
Hi Ty! Great question. What we do know is that the younger the individuals the better the results for conservative treatment. We know that before puberty the chest wall is more compliant. Not much research speaks on older individuals because usually we’ll see see surgery performed around ages 12-14 years old!
LikeLike
Great poster guys! Did the articles you researched say anything about an ideal age to start using the vacuum bell treatment for those with pectus excavatum?
LikeLike
Hi Lindsay! Great question. While the articles we looked through did not specify a certain age, they did mention that the younger the individual the better the vacuum bell results. Our one study had a median age of 14 but did not give us a break down of each participant’s age. So based on what we found, the younger the patient and the sooner they can start the vacuum bell treatment, the better the PE results!
LikeLike
Wow I found it super interesting that your research didn’t support PT as an individual intervention! I also found I interesting that your research showed that PE had little effects on the cardiopulmonary systems because that is the class that I learned it from. What are some of the critical problems to the thoracic cavity that your research mentioned regarding PE besides cosmetic effects? In my opinion, the cosmesis is very important to consider with these patients as they are younger in age and can be very affected by appearances and how others will see them. Great work on this poster guys, very interesting!!
LikeLike
Hey Alysa! Thanks for the question. We were hoping to find more literature that supported PT as an intervention as well, but unfortunately this is an area that remains highly unstudied. Depending on the severity of the deformity, PE can have adverse effects on the cardiopulmonary system. When researching this topic, we found that severe PE may compress the heart and lungs and lead to symptoms such as activity intolerance, increased heart rate & decreased cardiac output, irregular heart rate, shortness of breath, and chest pain.
LikeLike
First off, great job on the poster! Throughout your research, did you find anything that discussed pain management for these patients? I would imagine that the vacuum bell could be pretty discomforting. Second question (and kind of random), you mentioned that professional experience is key factor in applying the vacuum bell, do you know where PTs gain this experience, or is this something that is physician directed? Super random question, but this is some pretty interesting stuff. Great job!
LikeLike
Hey, Colton thank you for your questions. Unfortunately, we did not come across any pain management strategies for patients utilizing the vacuum bell in our research which is tough because like you stated the vacuum bell can be very uncomfortable especially for younger children that may not fully understand the process. Our research did mention that intense pain from the vacuum bell should not be occurring and it should be more of a pressure-type sensation. If pain greater than the pressure feeling is occurring the patient or patient representative should consult the professional that implemented the treatment plan. I believe that this is a treatment that would require a lot of education and monitoring to ensure safe and effective use. To answer your second question, the first initiation of the vacuum bell treatment would be implemented by a physician and all concerns or questions would go through them. Further education and assistance with the vacuum bell could come from a therapist but should also be communicated with the physician that prescribed it. Therapists could always learn more about the vacuum bell through research or by reaching out to other clinicians that provide the treatment to get more experience. Therapists will play a bigger role in implementing some of the diaphragmatic breathing, box breathing, thoracic spine, and rib cage mobilizations, strengthening of paraspinal and periscapular musculature that Kristi had mentioned in the first question.
LikeLike
Great work on your project! It was very interesting and informative. Based on your finding from your poster, it is clear than more research is needing to be done on PE. How do you see this being done? For example, would a case study be beneficial or some other type of research design? Also, what other alternative treatments do you think would be beneficial for this population that could be studied?
LikeLike
Thank you Brooke for the questions! Yes, much more research and awareness of chest wall deformities are necessary to help find more conservative options for pectus excavatum treatment. Although a randomized control trial would be the best study results-wise, it would be unethical to treat one kiddo with conservative treatment and one with non-conservative just for research purposes. It would be a very difficult study to conduct and to do fairly. I believe that this early in conservative treatment techniques more case studies would be beneficial just to get more of an idea of beneficial conservative treatments for kiddos. Other alternative treatments besides bracing and suction/compression are really difficult to come up with due to the fact it is more of a skeletal issue than a muscle issue and it’s hard to change that without some sort of bracing or suctioning pressure device. I do believe it would be beneficial for more research to be conducted on physical therapy interventions such as mentioned in the first answer by Kristi (breathing techniques, thoracic spine, and rib cage mobilizations, and strengthening paraspinal and periscapular musculature). Although physical therapy may not completely fix the deformity it may help prevent secondary complications. It is a tough diagnosis to come up with easy fixes, but I think continued research and advances with the vacuum bell and physical therapy would both be highly beneficial.
LikeLike
Nice job on the poster guys! It seems crazy to me that if a child has PE there are so few conservative options and at this time not many seem to be supported by literature. Your group mentioned a dynamic chest compressor orthosis. When conducting research did you happen to read anything related to this device and its potential for benefiting kiddos with PE?
LikeLike
Hi Jordyn! Thanks for the question. Most of the research we found on conservative treatments for PE was centered around the vacuum bell. We did find an article that used a dynamic chest compressor to treat pectus deformities. This device would be used in mild to moderate cases when the child is young enough to still have a flexible chest wall. My understanding is that this device is mostly used in the treatment of pectus carinatum, which is characterized by chest wall protrusion, instead of depression like in PE. The brace applies pressure centrally on the sternum to decrease the severity of the chest protrusion. The same process can be used to treat PE as well, but using this device can result in an overcorrection of the deformity due to the flexibility of the chest wall in immature patients. The dynamic chest compressor requires increased patient compliance and motivation as a daily exercise routine is performed to encourage lung expansion against the chest wall, helping to push it outwards. For young children, completing these exercises daily may be difficult unless they have encouragement from their families. The dynamic chest compressor would be a good conservative treatment option for those patients that are highly motivated.
LikeLike
Awesome job, guys. You stated on the poster that individuals with PE may experience worsening symptoms as the chest wall becomes stiffer (I’m assuming this is age related), but also note that mild PE is mostly cosmetic. My questions are, were there any numbers given as to how prevalent moderate to severe PE is and what the percentage is of those who are in need of surgical/PT intervention?
LikeLike
Thanks for the question Ryan. The prevalence of PE is estimated to be about 1:300-400 people and result in approximately 90% of all chest wall deformities. Another small percentage of chest wall deformities include pectus carinatum which would be a convex deformity with a barrel/pigeon look. No exact numbers were given on the prevalence between mild, moderate, and severe cases of PE. From our research, we know that surgical intervention is typically required for moderate to severe PE as indicated by a Haller index of 3.2 or greater and conservative options such as PT and/or the vacuum bell will be more appropriate for cases with a Haller index less than 3.2.
LikeLike